Medical Pharmacology Chapter 46: Congestive Heart Failure
|
|
Medical Pharmacology Chapter 46: Congestive Heart Failure
|
|
|
|
|
Clinical Manifestations and Physical Findings in Congestive Heart Failure
Dyspnea: The most common symptom of heart failure, dyspnea or respiratory distress occurs because of increased effort of breathing.
Dyspnea occurs initially upon exertion, but in advanced CHF may occur at rest.
Cardiac dypsnea is usually seen in patients with increased pulmonary venous and capillary pressure.
The combination of interstitial pulmonary edema and vessel enlargement result in reduced lung compliance and increased respiratory muscle work of breathing.
Enhanced activity of respiratory muscles further compromise available oxygen and contributes to the sensation of breathlessness.
Orthopnea, dyspnea while recumbent, is due fluid redistribution from the lower extremities into the chest with a resultant increase in pulmonary capillary hydrostatic pressure.
Paroxysmal (nocturnal) dyspnea is a sudden-onset of severe shortness of breath and coughing, awakening the patient.
Factors that produce paroxysmal dyspnea include:
Depression of respiratory center during sleep (decreases arterial oxygen)
Decreased ventricular function due to decreased sympathetic tone (decrease myocardial contractility and hence cardiac output) and
Redistribution of fluid to the chest.
|
|
|
|
|
|
Cardiac asthma, related to paroxysmal dyspnea, is characterized by wheezing due to bronchospasm.
Acute pulmonary edema, however, involves a significant elevation of pulmonary capillary pressure leading to alveolar edema, extreme shortness of breath and rales.
Expectoration of blood-tinged fluid may occur.
Acute pulmonary edema may be fatal.
Fatigue, weakness and reduced exercise capacity are common in congestive heart failure patients.
Exercise capacity is reduced because increased cardiac output required to support increased levels of physical activity is unavailable or inadequate.
Pulmonary Rales
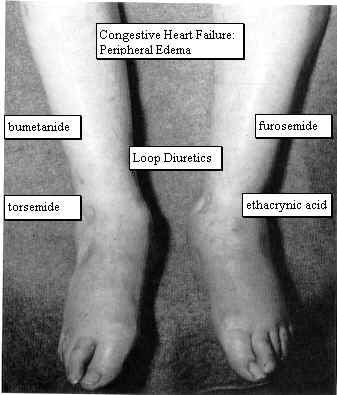
Peripheral (cardiac) edema is commonly seen symmetrically in the legs, particular in the pretibial region and ankles.
|
|
|
Ascites and pleural effusion.
Pleural effusion results from increased pulmonary capillary hydrostatic pressure and the attendant movement of fluid into the pleural cavity.
Congestive Hepatomegaly
Jaundice
|
Increased circulating tumor necrosis factor |
Increased metabolic rate need to support the increased effort of breathing |
Anorexia, nausea, vomiting due to digitalis intoxication, congestive |
|
Hepatomegaly, and abdominal fullness |
Impairment of intestinal absorption due to intestinal venous congestion |
Protein-losing enteropathy (rare) |
|
The fundamental abnormality in heart failure is embodied in:
|
|
Figures from "Harrison's Principles of Internal Medicine", Thirteenth Edition, pages 995 and 996. |
|
Factors Influencing Cardiac performance and Output
Ventricular end-diastolic volume (preload)
Atrial contraction
Inotropic state (myocardial contractility)
Ventricular afterload
Exercise
Ventricular end-diastolic volume (preload)
For any given inotropic state, ventricular performance will be significantly affected by the degree of ventricular stretch as determined by ventricular end-diastolic volumes (EDV).
The general relationship, as shown above, is the Frank-Starling mechanism.
Several factors influence end diastolic volumes, beginning with total blood volume.
Significant volume depletion leads to decreased cardiac output with preload and end-diastolic volumes declining (NPO, fluid replacement).
Blood volume distribution is important. Factors that affect distribution include:
Body position: gravitational forces, in the upright individual, results in pooling to extrathoracic compartments, especially the legs.
By contrast, in the recumbent individual, blood will redistribute into the thorax, increasing preload.
Venous tone:
Venular smooth muscle tone is under sympathetic neural and humoral control.
Exercise or hypotension result in venoconstriction and an increase in intrathoracic, intraventricular blood volume.
Accordingly, these conditions increase cardiac output by increasing end-diastolic volumes.
Skeletal muscle activity: During exercise, blood is displaced from the periphery due to the squeezing action of contracting muscle on the venous bed. Increased preload results as does increased cardiac output and work.
Atrial Contraction
Atrial contraction (atrial kick) enhances ventricular filling.
In the hypertrophic ventricle (with reduced compliance) appropriately timed atrial contraction may be especially important in achieving adequate levels of ventricular filling.
Increased heart rate (reduced filling times) or atrial arrhythmias reduce or eliminate the effectiveness of atrial kick.
|
|
|
|
|
1Weinberger, H., Diagnosis and Treatment of Diastolic Heart Failure, Hospital Practice
2Liggett SB, Wagoner LE, Craft LL, Hornung RW, Hoit BD, McIntosh TC, Walsh RA. The Ile164 beta2-adrenergic receptor polymorphism adversely affects the outcome of congestive heart failure. J Clin Invest 102:1534-1539, 1998.
3Moore JD, Mason DA, Green SA, Hsu J, Liggett SB. Racial differences in the frequencies of cardiac beta1-adrenergic receptor polymorphisms: analysis of c145A>G and c1165G>C. Human Mutation 14(3):271, 1999.
4Mason DA, Moore JD, Green SA, Liggett SB. A gain-of-function polymorphism in a G-protein coupling domain of the human beta1-adrenergic receptor. J Biol Chem 274:12670-12674, 1999.
5Spencer, K.T. and Lang, R.M. Kirk T. Spencer, MD Roberto M. Lang, MD, Diastolic heart failure, What primary care physicians need to know , vol. 101, no. 1, January 1997, Postgraduate medicine
6Aronow WS, Ahn C, Kronzon I. Prognosis of congestive heart failure in elderly patients with normal versus abnormal left ventricular systolic function associated with coronary artery disease. Am J Cardiol 1990;66(17):1257-9
7Takarada A, Kurogane H, Minamiji K, et al. Congestive heart failure in the elderly-echocardiographic insights. Jpn Circ J 1992;56(6):527-34
8.Iriarte M, Murga N, Sagastagoitia D, et al. Congestive heart failure from left ventricular dysfunction in systemic hypertension. Am J Cardiol 1993;71(4):308-312
9.Madsen BK, Hansen JF, Stokholm KH, et al. Chronic congestive heart failure: description and survival of 190 consecutive patients with a diagnosis of chronic congestive heart failure based on clinical signs and symptoms. Eur Heart J 1994;15(3):303-10
10Iwase M, Nagata K, Izawa H, et al. Age-related changes in left and right ventricular filling velocity profiles and their relationship in normal subjects. Am Heart J 1993;126(2):419-26
11Klein AL, Burstow DJ, Tajik AJ, et al. Effects of age on left ventricular dimensions and filling dynamics in 117 normal persons. Mayo Clin Proc 1994;69(3):212-24
12Zile MR: Diastolic dysfunction: Detection, consequences, and treatment. Part I: Definition and determinants of diastolic function. Mod Concepts Cardiovasc Dis 58:67, 1989
13Kitzman DW et al: Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: Failure of the Frank-Starling mechanism. J Am Coll Cardiol 17:1065, 1991
General References
Hollenberg, S.M. and Parrillo, J.E., Shock, In Harrison's Principles of Internal Medicine 14th edition, (Isselbacher, K.J., Braunwald, E., Wilson, J.D., Martin, J.B., Fauci, A.S. and Kasper, D.L., eds) McGraw-Hill, Inc (Health Professions Division), 1998, p. 215-222
Hoffman, B.B and Lefkowitz, R.J, Catecholamines, Sympathomimetic Drugs, and Adrenergic Receptor Antagonists, In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) The McGraw-Hill Companies, Inc.,1996, pp.222-224.
Stoelting, R.K., "Sympathomimetics", in Pharmacology and Physiology in Anesthetic Practice, Lippincott-Raven Publishers, 1999, p.259.
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |