Mortality from elective abdominal
aneurysm surgery: about 8% (twofold higher than that
associated with occlusive major vascular disease)
Approximate median survival following
surgery:
abdominal aneurysmal repair: about 6
years
aorticoiliac revascularization: about 11
years
Basis for Morbidity/ mortality:
Secondary to myocardial dysfunction
(correlation may be as high as 100% -- death due to cardiac
disease)
Conservative treatment, i.e. observing
aneurysmal growth until size becomes > 6 cm, has NOT been
well accepted despite relatively high surgical risk
Since 1990, perioperative mortality has
declined; however high mortality (45%-90%) continues to be
associated with emergency surgery for ruptured aneurysm
Predicting which patients will suffer in
aneurysmal rupture: unreliable
Patients undergoing aneurysmal surgery tend
to be older (10 years) than patients undergoing aortic
revascularization.
Older patients tend to higher risk of
adverse outcome; after correcting for age, life expectancy
following aneurysmal surgery is less than that for
revascularization.
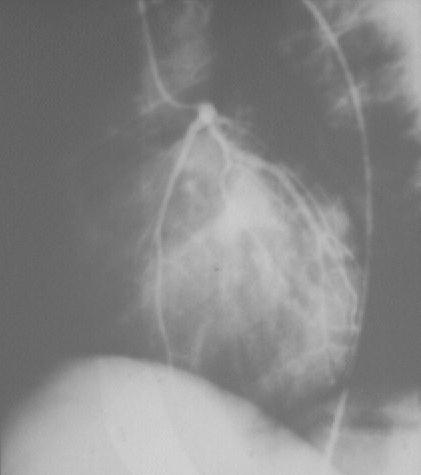
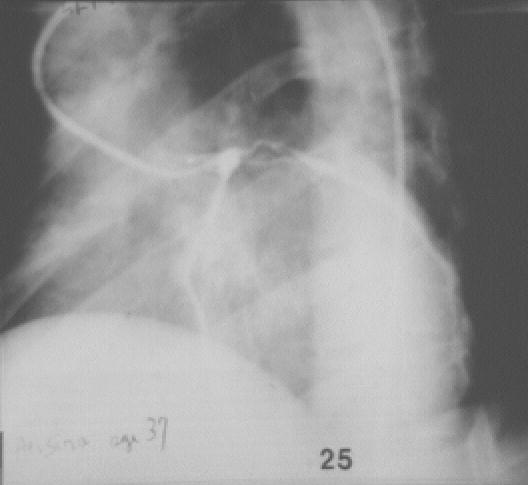
"Normal left coronary angiogram.
Left anterior oblique view (45 degrees) (Left); Left coronary
angiogram. Left anterior oblique view. Narrow area from
disease proximal end of circumflex and top of anterior
descending. Male age 37. Severe angina not controlled by
medical treatment": courtesy of SouthBank University, London;
used with permission
Most patients undergoing aortic
reconstruction had clinical evidence of coronary vascular disease
Strongest preoperative indicator of
postoperative my guarded complications was the presence of both
preexisting cardiac disease and diabetes
Age: Significant increase in risk
with increasing age
Greater effect on mortality than
coronary vascular disease presents or aortic aneurysm rupture
history
Renal Disease/Failure
Factors that increase
mortality risk:
Postoperative renal failure
(if serious enough to record analysis)
Preexisting renal disease
Factors that decreased
risk:
improved intravascular volume
management by anesthesia providers
Smoking
and pulmonary disease
Unclear relationship between
smoking and vascular surgery outcome
Smoking increases
respiratory complications following bypass surgery
Smoking cessation two months
before surgery may reduce risk for complications by 66%
(compared to patients who stop smoking < two months before
the procedure)
Diabetes mellitus
Diabetic patients are
usually classified as type III, associated with a reduced five-year
survival rates ( 65%,secondary to small vessel disease)
Also associated with increased
likelihood of surgical wound complication.
Primary Reference: Katz, J., Evaluation
Risk Assessment of Patients with Vascular Disease in Principles
and Practice of Anesthesiology (Longnecker, D.E., Tinker, J.H.
Morgan, Jr., G. E., eds) Mosby, St. Louis, Mo., pp. 201-218,
1998.