|
|
|
|
|
|
|
Medical Pharmacology Chapter 29: Diabetes
|
|
|
|
|
|
|
Diabetes
 |
|
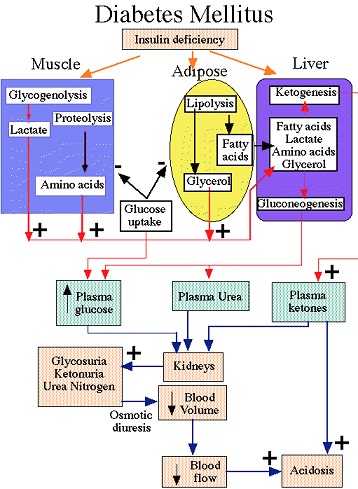
Diabetes mellitus is the most important disease involving endocrine pancreas.
Major manifestations:
inappropriate hyperglycemia
metabolic disorders
Two types:
Type I diabetes: insulin-dependent diabetes mellitus (IDDM)
Type II diabetes: non-insulin dependent diabetes mellitus (NIDDM)
The severe form may be associated with ketosis if untreated.
Usually juvenile in onset, but occasionally adult onset.
Insulin nearly absent
Plasma glucagon elevated
Pancreatic B cell is not responsive to insulinogenic stimuli.
Exogenous insulin required to:
Prevent ketosis
Reduce hyperglucagonemia
Reverse catabolic state
Infectious etiology possibly associated with a genetic predisposition.
Toxic environmental factor possibly also associated with a genetic predisposition.
Mumps virus
Coxsackievirus B4
Destructive cytotoxins and antibodies from sensitized immunocytes
Autoimmune component suggested given that pancreatic B cell damage is reduced when immunosuppressive drugs e.g. cyclosporine/azathioprine, are administered early in Type I diabetes.
Pancreatic tissue transplanted from a nondiabetic monozygotic twins into the diabetic twin is rapidly destroyed in absence of immunosuppression.
Immune system mediation of pancreatic beta cell obstruction (Type I diabetes)
Associated with other autoimmune endocrinopathies:
Adrenal insufficiency
Hashimoto's thyroiditis
Most patients have antibodies against insulin and other beta cell antigen.
![]() Pancreatic
beta cell destruction --
development of
insulin-dependent
diabetes mellitus
Pancreatic
beta cell destruction --
development of
insulin-dependent
diabetes mellitus
Slow loss of insulin reserve
Islet cell tumor on a development (normal glucose; normal glucose tolerance; normal insulin response to glucose load)
Decreased glucose tolerance (fasting blood glucose: normal; last prediabetic phase)
Fasting hyperglycemia (no ketosis, even with poorly control diabetes)-- looks like NIDDM
Insulin-dependent stage -- ketoacidosis occurs, especially following stress (in this point life-long insulin therapy is required or pancreatic transplant)
Immune-directed pancreatic beta cell destruction
Humoral and cell-mediated processes (cell-mediated mechanisms more important)
Islet cell antibodies: -- antibodies against:
Insulin
Proinsulin
Glutamic acid decarboxylase (two forms)
Ganglioside ganglioside antigens
Immune cell involvement:
Activated cytotoxic T lymphocytes (CD8+)
Macrophages
Releases cytokines (interleukin 1, tumor necrosis factor alpha, a.k.a., TNF-α.
By the time overt diabetes clinically presents, most insulin-producing cells have been destroyed.
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |