Increased
intraoperative blood-pressure lability in patients not receiving
their antihypertensive medication: Recommendation -- administer
medications on the day of surgery
-- Exception: possibly diuretics
Concerning elective surgery in
patients with uncontrolled hypertension:
Surgery not associated with elevated incidence of perioperative
cardiac morbidity if preoperative diastolic pressures were less
than 110 mm Hg with careful perioperative blood-pressure
monitoring
Preoperative
approaches to the hypertensive patients:
Factors that increased risk of
myocardial ischemia intraoperatively
uncontrolled hypertension or
hypertension control solely with diuretics {compared to
patients treated with atenolol (Tenormin)}
myocardial ischemia --most
likely occurs during:
intubation
emergence from anesthesia
Intraoperative ischemia: primary
association = tachycardia
Special
considerations:
Diabetic patients with hypertension (noncardiac surgical
procedures)
Intraoperatively events predictive of postoperative
for cardiovascular complications {renal/cardiac morbidity}
intraoperative
hypotension (> 20 mm Hg decrease in mean arterial
pressure (duration > 1 hour))
intraoperative
hypertension (> 20 mm Hg increased in mean arterial
pressure (duration > 15 minutes )) alternating
with hypotension
Hypertension & organ transplantation
Occurs only in some patients
Hypertension increases the likelihood of renal failure in
the transplanted kidney
Antihypertensive drug treatment: no improvement in graft
survival
Post-organ transplantation
hypertension probably due to immunosuppressive drugs:
Glucocorticoids
-- Na+/H2O retention
Cyclosporine
(Sandimmune, Neoral): increased sympathetic nervous
system activity (suggested factor)
Perioperative
issues in managing patients with cerebrovascular
disease/hypertension:
Aneurysmal subarachnoid hemorrhage patients
Hypertension management may reduce re-bleeding
Hypertension
management, however may increase cerebral infarction risk
Surgical intervention for aneurysmal subarachnoid hemorrhage
in patients who have had hypertension is associated with
increased seizure risk.
Diastolic pressures: best maintained in a range of
95-105 mm Hg
Post-operative control of BP & vasospasm--
nimodipine (Nimotop)
Nimodipine (Nimotop)
Overview
Highly lipid-soluble
nefedipine analog
Lipid solubility promotes CNS access
where the drug reduces large cerebral arterial
contraction
Clinical Use:
Cerebral
Vasospasm:
Useful in
preventing/reducing cerebral
vasospasm associated with
subarachnoid hemorrhage
Vasospasm
-- mediated by calcium ion influx
Nimodipine (Nimotop)
administered over a three week
course (oral administration)
results and decreased frequency
of neurologic effects secondary
to cerebral vasospasm in
subarachnoid hemorrhage patients.
For
comatose patients:
deliver through
nasogastric tube
nitroprusside
interacts with oxyhemoglobin,
forming methemoglobin with
cyanide ion and nitric oxide (NO)
release
NO activates
guanylyl cyclase (in vascular
smooth muscle);resulting in
increased intracellular cGMP
cGMP
inhibits calcium entry into
vascular smooth muscle (may also
increase calcium uptake by smooth
endoplasmic reticulum): producing
vasodilation
Mechanisms by which cGMP relaxes
vascular smooth muscle remain to be
elucidated. cGMP does, however,activate K+
channels (hyperpolarizing effect),
activate a cGMP-dependent protein kinase, , decrease IP3, and inhibit calcium entry into the smooth muscle cells.
NO: active
mediator responsible for direct
nitroprusside vasodilating
effect.
Note that
organic nitrates (e.g.
nitroglycerin) require
thio-containing agents to
generate NO
The reaction: nitroprusside interacts
with oxyhemoglobin, leading to methemoglobin
formation with
cyanide ion and nitric oxide (NO)
release produces an unstable
nitroprusside radical
nitroprusside
radicals decomposes releasing
five cyanide ions (one cyanide
reacts with methemoglobin to form
cyanomethemoglobin)
remaining free cyanide
ions (following reaction with
hepatic & renal rhodanase)
are converted to thiocyanate
{thiosulfate donor: body sulfur
stores are sufficient detoxifying
about 50 milligrams nitroprusside})
Positive
inotropic &
chronotropic responses:
reflex-mediated secondary
to hypotensive response
Net
increase in cardiac
output due to:
increase contractility
decreased left
ventricular ejection
impedance
Hypotensive
response: associated with
reduced renal function;
renin release occurs
(explains over shoot upon
nitroprusside
discontinuation {ACE
inhibitor-sensitive, i.e. an ACE inhibitor
will prevent this overshoot effect})
Nitroprusside: may worsen
myocardial infarction
damage due to
"coronary
steal", blood flow directed away from
ischemic areas by
arteriolar vasodilation
Cerebrovascular Effects:
Increased
cerebral blood flow,
volume.
with
decreased intracranial compliance,
increased
intracranial pressure results
Generally,
increases in intracranial
pressure are most
apparent when systemic
mean arterial pressure
decreases by less than
30%
if
systemic mean arterial
pressure decreases by
> 30%, intracranial
pressure decreases below
the awake level.
Nitroprusside
contraindicated in
patients with known
inadequate cerebral blood
flow (e.g. high
intracranial pressure;
carotid artery stenosis)
Hypoxic Pulmonary
Vasoconstriction
Nitroprusside
infusion (and other
vasodilators) causes
decrease in PaO2
Mechanism:
vasodilator-mediated
reduction in hypoxic
pulmonary
vasoconstriction
Rapid,
predictable vasodilation
& decrease in BP
allows a nearly bloodless
surgical field, required
in some operations: spine
surgery, neurosurgery
(also reduces
transfusions)
Other
drugs that might be
chosen to produce
controlled hypotension,
nitroprusside is most
likely to ensure adequate
cerebral perfusion (mean
arterial pressure's of
50-60 mm Hg can be
maintained without
apparent complications
{in healthy patients})
The
potential for cyanide
toxicity can be
diminished by:
Use of other
cardiovascular depressant
drugs which reduce
nitroprusside
requirements
These drugs include:
volatile anesthetics,
beta-adrenergic
antagonists, calcium
channel blockers; note
that beta adrenergic
antagonists may cause a
decreased cardiac
output-- a potential
problem in patients with
diminished the
ventricular reserve.
Treatment of
hypertensive emergencies
Acute &
chronic heart failure
Reduction
of afterload may be
important for patients
with CHF, mitral or
aortic regurgitation,
acute myocardial
infarction with left
ventricular failure
Role of
nitroprusside in chronic,
congestive heart failure
-- advantageous because:
reduced
ventricular ejection
impedance (injection at
lower end-diastolic
volumes
preload
reduction (secondary to
blood pooling in venous
capacitance vessels --
reflected in decreased
ventricular and-diastolic
volume)
Surgical
indications:
Aortic
surgery
reduction
of proximal hypertension
associated with aortic
cross-clamping (thoracic
aortic aneurysm, dissections,
coarctations)
distal
hypotension may occur
(relative to clamp
location)
Cardiac surgery
necessitating
cardiopulmonary bypass
Activation of
renin-angiotensin system
may cause systemic
hypertension during
cardiac surgery
Nitroprusside is
effective in reducing
such increases in BP
Following cardiopulmonary
bypass {re-warming
phase}, nitroprusside-mediated
vasodilation facilitates
heat delivery to tissues
{reduces nasopharyngeal
temperature decline after
bypass}
Nitroprusside is
effective in managing
pulmonary hypertension
after valve replacement
Vasodilators
used for acute management of hypertensive crisis
or malignant hypertension include sodium
nitroprusside and diazoxide.
Nitroprusside
sodium (Nipride) is the agent of choice--
advantages
Rapid onset
Effect diminishes
rapidly upon drug discontinuation
May also be used
(rapid injection) to reduce
systemic blood-pressure
associated with direct
laryngoscopic tracheal intubation
Administered by a
continuously variable rate i.v. infusion
pump, precise blood pressure control can
be obtained.
Nitroprusside sodium
(Nipride), a nitrovasodilator, is
metabolized by smooth muscle cells to
nitric oxide which dilates both
arterioles and venules.
If patients have controlled
hypertension, anxiolytics may be appropriate {preoperative
medication}
diazepam (Valium); oral
midazolam (Versed); intramuscular
Patients managed with diuretic
drugs for hypertension:
Diuretics not given on same day of surgery
Patients may be volume depleted
Patients whose hypertension is managed with diuretics may have
to be dehydrated prior to the surgical procedure
{remaining antihypertensive medications, i.e. non-diuretics
should be administered on the surgical day.}
Management of hemodynamic variability
during anesthetic induction/emergence:
Effective in management
of sinus tachyarrhythmias & hypertension in cardiac
& noncardiac surgical patients
Lidocaine (Xylocaine)
Nicardipine (Cardene)-management
of perioperative hypertension
Choice of anesthetic for maintenance:
Any agent reasonable except for
ketamine (Ketalar)
Ketamine (Ketalar) associated
with hypertension, increased intracranial pressure &
tachycardia
Intraoperative
management of acute blood pressure increases:
Prior
to antihypertensive drug administration, rule out:
hypoxemia
hypercarbia
inadequate anesthetic depth
Hulyalkar, A. R., and Miller, E.D., Evaluation of the
Hypertensive Patient in Principles and Practice of Anesthesiology (Longnecker,
D.E., Tinker, J.H. Morgan, Jr., G. E., eds) Mosby, St. Louis,
Mo., pp. 157-165, 1998.
Stoelting, R.K., "Calcium Channel
Blockers", in Pharmacology and Physiology in Anesthetic Practice,
Lippincott-Raven Publishers, 1999, p. 350.
Stoelting, R.K., "Antihypertensive Drugs",
in Pharmacology and Physiology in Anesthetic Practice, Lippincott-Raven
Publishers, 1999, 302-312;and "Peripheral Vasodilators", in
Pharmacology and Physiology in Anesthetic Practice, Lippincott-Raven
Publishers, 1999, 315-322.
Control of other risk factors
(blood lipids, smoking)
Diet involves
several aspects that may include:
reduction of sodium intake
caloric restriction for obese
patients
restriction of cholesterol
and saturated fat intake.
Pharmacological Management
Pharmacological interventions in
essential hypertension management is
based on selecting often a single initial
agent and evaluation of patient response.
Unless clinical conditions require
immediate reduction in blood pressure as
in hypertensive crisis, the first
step may involve the use of :
a calcium channel
blocker or beta-blocker, or
angiotensin converting enzyme
inhibitor (ACE inhibitor). The
specific clinical presentation
may favor one choice over
another.
For example, in patients with
asthma or chronic obstructive pulmonary disease (COPD) the use of a beta-adrenoceptor
antagonist may be contraindicated since agents
belonging to this drug class may cause
bronchoconstriction.
Alternatively, a patient with marginal
left ventricular function, predisposed to
congestive heart failure, may not tolerate
beta-blockers or calcium channel blockers because
both mediate a negative inotropic effect
(reduced myocardial contractility). At this step,
beginning with a low dosage first is usually
appropriate.
Thiazide diuretics has been often
used in the past as the first drug given.
Thiazides may be added if
adequate blood pressure control by a
calcium-channel blocker, a beta-blocker,
or an ACE inhibitor has not been
achieved.
Thiazides promote
potassium loss and increases in serum
lipids.
If control has not been achieve
with the above drugs at optimal dosages, a antiadrenergic drug may be added
(such as a central or peripheral-acting
sympatholyic). Peripheral vasodilators may also
be used at this stage.
The general idea
is to use a single agent before progressing to
multiple agents and then stronger multiple drugs.
Often the side-effect profile becomes less
favorable as more and stronger drugs are added.
Antihypertensive
Medication Sequence
Note the
progression of antihypertensive medication
beginning with a low dosage of
either an ACE inhibitor, calcium channel blocker
or beta blocker
and proceeding, if needed to add a
diuretic
and ultimately additional more
powerful drugs, such as centrally acting
sympatholytics, peripheral vasodilators or
combination.
At
each step dosages are reviewed and if the patient's
hypertension is controlled then therapy may be continued
with review for possible removal of medication.
Figure adapted from Harrison's
"Principles of Internal Medicine, Thirteenth
Edition, p. 1128
For hypertensive emergencies/crises
sodium nitroprusside is the agent of first
choice.
Hypertensive Crisis
Definition: diastolic
pressure > 130 mm Hg
Malignant hypertension (evidence of end-organ
damage): Medical emergency-requires immediate treatment
Malignant
hypertension requires the use of parenteral agents with
intra-arterial BP monitoring
Without end-organ damage present, oral or
sublingual antihypertensive drugs might be used
Factors causing a rapid increase in
BP:
Elevation of intracranial pressure (increased
blood pressure allows maintenance of cerebral perfusion)
Neurological causes of hypertensive crisis:
intracranial hemorrhage
head trauma
CNS tumor
thromboembolic stroke
subarachnoid hemorrhage
Cautious management for patients with
hypertensive crisis -- and hypertensive drugs given in severe
hypertension (> 200/130 mm Hg)
Nitroprusside sodium (Nipride) -- careful
administration {may increase
intracranial pressure and patients with reduced intracranial
compliance)
Beta adrenergic receptor blocking drugs:
Not recommended; may cause cerebral vasospasm
Centrally acting drugs {e.g., clonidine (Catapres);
methyldopa (Aldomet)}: not recommended for hypertensive
crisis as a result of neurological cause
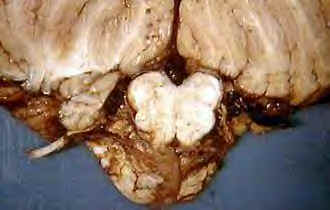
Hemorrhage, Subarachnoid, Hypertensive
Vessels (left); Hemorrhage, Intraventricular Medulla, Extension
into Lateral Recess and Subarachnoid Space (right): Courtesy of Digital Slice of Life (http://medstat.med.utah.edu/kw/sol/sss/index.html)
Cardiovascular
causes of hypertensive crisis:
Myocardial
infarction
Dissecting
aortic aneurysm
Therapeutic
Objectives:
20%-25% reduction in diastolic or pressure (100 mm Hg)
For dissecting aortic aneurysm cases, reducing the arterial
pressure rate of rise may prevent aneurysmal rupture-{nitroprusside
sodium (Nipride) + ß-adrenoceptor blocker is a useful
combination}
In myocardial infarction,
maintenance of coronary
perfusion is critical as systemic pressure is reduced-Useful
drugs include:
nitroglycerin
calcium channel blockers
ß adrenoceptor blockers
Renal causes of hypertensive
crisis:
Renal
artery stenosis
Parenchymal
renal disease
Therapeutic
objectives:
maintain renal perfusion while decreasing
BP to prevent fibrinoid necrosis
Useful
drugs:
Nitroprusside sodium (Nipride)
Calcium channel blockers
Other interventions:
the combination of renal failure &
malignant hypertension may require dialysis
Special cautions:
Thiocyanate levels must be monitored when
nitroprusside sodium (Nipride) is used at high doses for
extended periods of time
ACE inhibitors should not be used if
bilateral renal artery stenosis suspected/confirmed:
Mechanism -- glomerular filtration is
dependent on post-glomerular arteriolar constriction,
which is maintained by angiotensin II. Renal failure can
be induced if post-glomerular arterial constriction is
lost.
Other causes of hypertensive
crisis:
Ingestion of tyramine-rich foods in patients taking MAO
inhibitors
Preeclampsia
Recreational drug use
Hyperautonomic syndromes {chronic smoke or dysfunction}
Pheochromocytoma-massive release of endogenous catecholamines by
tumor.
CT imaging: Right Renal Artery Stenosis
(left); bilateral Renal Artery Stenosis (right)-(http://www.ctisus.org/angioatlas/abdominal/2_ras5a.html)
used with permission
Hulyalkar, A. R., and Miller, E.D.,
Evaluation of the Hypertensive Patient in Principles and Practice of
Anesthesiology (Longnecker, D.E., Tinker, J.H. Morgan, Jr., G. E., eds)
Mosby, St. Louis, Mo., pp. 157-165, 1998.