|
|
|
|
|
|
|
Nursing Pharmacology: Antiviral Drugs
|
|
|
|
|
|
|
Antiviral Drugs
Introduction: Influenza is described as an acute respiratory infection due to influenza viruses.2
|
 |
|
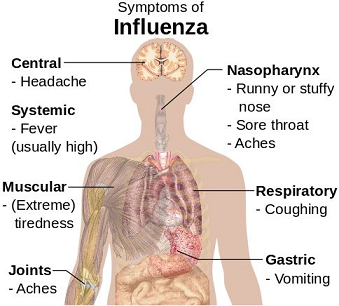
The upper and/or lower respiratory tract is affected with systemic presentations including fever, myalgia (muscle aches), headache and weakness.
 |
|
Outbreaks are often yearly and may result in both notable morbidity and even mortality rates in certain high-risk individuals.2
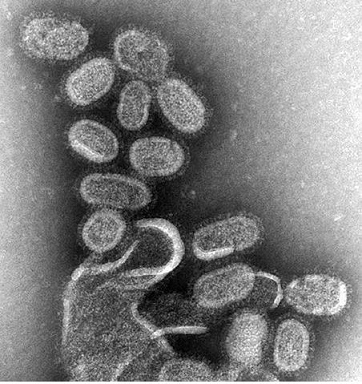
Influenza viruses belong to the Orthomyxoviridae family.2
|
Often the term "flu" is used in reference to a relatively mild upper respiratory infection, perhaps the "common cold". 2
This illness is not due to influenza virus but rather other upper respiratory viruses, such as rhinoviruses.
![]() Influenza is notably a severe, acute disease across age groups with
symptoms as noted below.
Influenza is notably a severe, acute disease across age groups with
symptoms as noted below.
The acute initial stage of influenza last about three days although cough and other symptoms may endure for several weeks.2
|
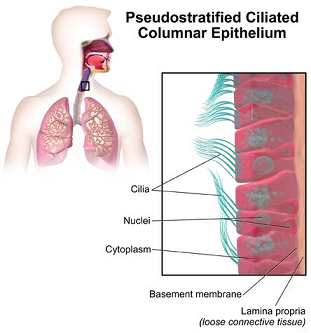
Influenza virus initially infects upper respiratory tract epithelial cells, causing a loss of ciliated epithelium.2
|
|
|
|
|
|
Loss of ciliated epithelium in turn prevents the respiratory tract from clearing viruses or bacteria by the process of mucociliary flow.2
Production of interferons, cytokines and other response factors promotes both local and systemic inflammatory reactions.2
Systemic inflammatory effects form the basis of many "flu" symptoms that comprises syndrome (fever, chills, headache, malaise and muscle aches).
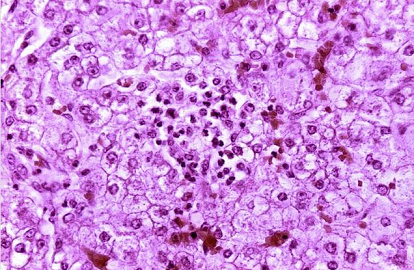
In addition absence of ciliated epithelium allows bacteria to more readily enter the lower respiratory tract.
![]() Many
deaths thought to result from influenza virus infection may
be due to secondary bacterial pneumonias.2
Many
deaths thought to result from influenza virus infection may
be due to secondary bacterial pneumonias.2
Complications due to influenza are more likely to occur in patients older than 65 and in those individuals who also have chronic health issues.8
These health issues include:8
Cardiac disease
Congestive heart failure, as an example
Pulmonary disease
Chronic obstructive pulmonary disease (COPD)
Coronaviruses and rhinoviruses are the pathogens is most responsible for worsening of chronic lung disease.11
However, influenza might account for as much as 25%.11,12
Influenza virus and other respiratory viruses may worsen chronic respiratory diseases, by mechanisms likely associated with inflammatory mediators such as interleukins and cytokines and as a result of changes in the ratio of T-cell subsets, a change that may increase sensitivity to other allergens.11,13
Diabetes mellitus
Hemoglobinopathies
Renal disease
Immunosuppression.
Possible complications of influenza include myositis, sometimes with myoblobinemia and renal failure, myocariditis and pericarditis.10
Additional complications:
Encephalopathy
Transverse myelitis
Guillain-Barré syndrome and
Reye's syndrome (made more likely in children who have been administered aspiring have been noted.)
Reye's syndrome is a noninflammatory encephalopathy that develops acutely and is described by the:11
Clinical presentation overall and the finding that cerebrospinal fluid (CSF) contains < 8 m leukocyte/mm3 or by
Histological brain sections showing cerebral edema without perivascular meningeal inflammation associated with either fatty liver or a 3-fold increase in transaminases or serum ammonia.11,14
|
|
|
The correlation of Reye's syndrome with influenza has been suggested for several decades with more than 90% of cases occurring in white children less than 14 years of age.
Adult cases are typically associated with influenza A and appear fatal.11
Following severe viral pneumonia, some patients may experience additional, respiratory-related health issues including reactive airway disease, respiratory insufficiency and/or pulmonary fibrosis.10
The likelihood of influenza complications appears increased in second or third trimester pregnancy.
Another group at higher risk for influenza complications is children less than five years old, particularly infants.8
![]() The
most important influenza
complication is pneumonia including:
The
most important influenza
complication is pneumonia including:
"Primary" influenza viral pneumonia
|
|
|
|
|
Secondary bacterial pneumonia8,11
Viral influenza complicated by bacterial pneumonia was noted during the 1918 influenza pandemic as well as during subsequent epidemic and inter-epidemic periods.11,16
During the 1918 pandemic, S. aureus pneumonia was described.11,17
Features includeed:
Fulminant course with an "cherry-red indigo-blue" unusual cyanosis
Lack of consolidation
"Dirty salmon-pink purulent sputum"
Leukopenia
Multiple micro-abscesses described in autopsy
Near total fatality.
More recently, during the 2003-2004 and 2006-2007 influenza seasons, severe cases of community-acquired pneumonia caused by methicillin-resistant S aureus (MRSA) was associated with 33% mortality.11,18
In this circumstance the typical viral influenza infection proceeds to near resolution of symptoms only to be then complicated 4-14 days later by fever recurrence, dyspnea and pulmonary consolidation.
Typically pathogens responsible for this effect include Streptococcus pneumoniae, Staphylococcus aureus and Haemophilus influenzae along with some other Gram-negative bacilli.11
Streptococcus pneumoniae is likely the most notable pathogen responsible for secondary bacterial infection.
These bacteria colonize the nasopharynx and cause infection, given changes in bronchopulmonary defenses.8
The infection may be specified by Gram's staining along with culture of a sputum sample.
Secondary bacterial pneumonia is more likely to occur in high-risk patients with chronic pulmonary and cardiac disease and in elderly individuals.
Secondary bacterial pneumonia often responds to antibiotic therapy when treatment is begun promptly.8
Some mechanisms have been proposed that describe how bacteria act synergistically with influenza virus.11,19
These mechanisms include:
Increased binding and bacterial invasion
Enhanced viral replication
Changes in host-inflammatory response.
Interactions between influenza virus and bacteria have been described most thoroughly with Streptococcus pneumoniae.
In that instance, as viral neuraminidase cleaves sialic acid to release new virions from host cells, epithelial layer damage of the airways occurs which exposes binding sites required for pneumococcus adherence.11,19
Combination of viral and bacterial pneumonia.8
|
The most common pneumonia-related complication during influenza outbreaks suggests mixed features of both bacterial and viral pneumonia.8
Beginning with an acute illness, bacterial pneumonia manifestations become the prominent clinical presentation.8
Accordingly, sputum cultures during the viral/bacterial pneumonia timeframe contain both influenza A virus and a bacterial pathogen.
Physical examination and x-ray may reveal areas of consolidation or regions of infiltrates.
Mixed viral and bacterial pneumonia tend to have less widespread lung involvement compared to primary viral pneumonia.
As noted
earlier, bacterial infections typically respond to antibacterial drugs.8
![]()
![]()
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |