|
|
|
|
|
|
|
Nursing Pharmacology: Antiviral Drugs
|
|
|
|
|
|
|
Antiviral Drugs
Anti-viral drugs with activity against HIV (Human Immunodeficiency Virus)
HIV-1 Pathophysiology/Pathogenesis: HIV Disease Presentations
Heart disease has been identified in about 40% of autopsy cases (25%-75% considering various autopsy series) in HIV patients.2
During life, heart disease using echocardiography has been identified in about 25% of AIDS patients.
![]() In the early
stages of the HIV epidemic, cardiomyopathy (heart muscle disease) was
the major cardiovascular complication of HIV infection.2,9
In the early
stages of the HIV epidemic, cardiomyopathy (heart muscle disease) was
the major cardiovascular complication of HIV infection.2,9
Tuberculosis pericarditis, cardiomyopathy, pericardial effusion and pulmonary hypertension both initially and at the present time remain important cardiac diseases in Africa.
These presentations relate to the small number of patients (about 5%) who may have access to contemporary antiretroviral agents.
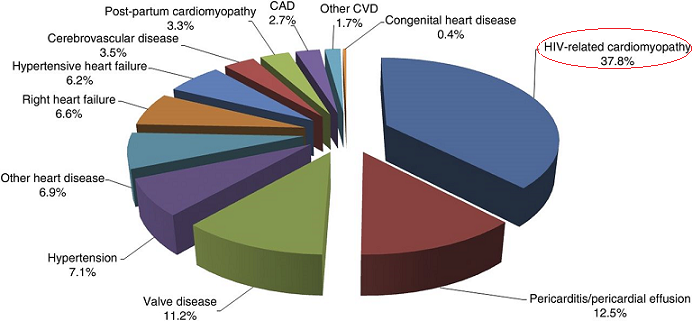
One of the major studies concerning the effects of HIV/AIDS on heart disease was conducted in South Africa.11
The study was known as the Heart of Soweto Study. In this prospective analysis of all de novo heart disease cases presented to the Cardiology Unit during 2006-2008 of the Chris Hani Baragwanath Hospital 5328 de novo heart disease cases were considered.11
About 10% of these cases (518/5328) represented HIV-positive patients and about half of these patients were given cART (HAART: highly active antiretroviral treatment) upon presentation.
The most frequently noted primary diagnosis related to HIV/AIDS was HIV-related cardiomyopathy (38% of the 518 patients).11
At present heart disease in HIV patients is now manifest in developed countries as coronary heart disease.2,9
The rate of myocardial infarction (MIs) is approximately 3.5/1000 patient-years. Furthermore, about 30% of these incidences were fatal.
The use of cART (HAART), highly active antiretrovirals, often consisting of two nucleoside reverse transcriptase inhibitors [NRTIs] along with one or two protease inhibitors appears to be the basis of the change in heart disease pattern since the beginning of the epidemic.
![]() cART-induced
metabolic abnormalities, especially insulin resistance and
hyperlipidemia appear important aspects of the problem.9
cART-induced
metabolic abnormalities, especially insulin resistance and
hyperlipidemia appear important aspects of the problem.9
Generally, in HIV patients, cardiovascular disease may be accounted for by expected risk factors including smoking, HIV infection-related, or complication of antiretroviral drugs.2
Patients with HIV infection exhibit both lower levels of high-density lipoprotein cholesterol (HDL, "good cholesterol") and higher levels of triglycerides; furthermore a higher incidence of smoking appears to be present in HIV-populations compared to comparable cohorts without HIV infection.
The rate of cardiovascular disease has been shown lower to be in patients treated with antiretroviral drugs.
![]() This finding
identified a relationship between HIV replication and cardiovascular
disease risk.2
This finding
identified a relationship between HIV replication and cardiovascular
disease risk.2
CD4+ T cell counts of <500/μl appears to be an independent risk factor for cardiovascular disease.
This risk factor appears comparable to the risk factor smoking.2
|
|
|
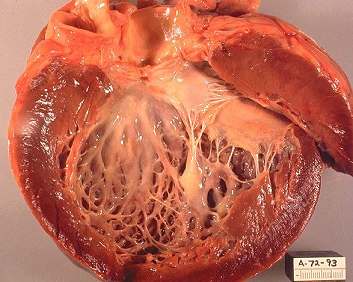
HIV-associated cardiomyopathy is characterized as a dilated cardiomyopathy presenting with congestive heart failure (CHF).2
 |
|
This cardiomyopathy occurs in the latter stages of HIV infection and histologically resembles myocarditis.
Dilated cardiomyopathy associated with HIV infection was initially described in 1986 and exhibits characteristics similar to idiopathic dilated cardiomyopathy in HIV-negative individuals.9
Associated isolated left ventricular dysfunction in HIV-AIDS patients may be due to a self-limiting myocarditis, since the dysfunction may resolve on its own.9
The differential diagnosis of cardiomyopathy in the HIV/AIDS setting takes into account:9
Left ventricular dysfunction due to ischemic heart disease
Hypertension
Diabetes
Coronary vasospasm (secondary to cocaine use) as well as
Drug hypersensitivity reactions.9
Heart muscle disease is associated with prevalence of about 4.5% for cardiomyopathy and 6.5% for left ventricular dysfunction.9
![]() These
conditions may present as clinical symptoms in about 6% of
HIV/AIDS patients.9
These
conditions may present as clinical symptoms in about 6% of
HIV/AIDS patients.9
![]() Cardiomyopathy has a poor prognosis, suggesting poor survival in
these patients when compared to similar patients with structurally
normal myocardium.9
Cardiomyopathy has a poor prognosis, suggesting poor survival in
these patients when compared to similar patients with structurally
normal myocardium.9
The HIV cardiomyopathy-associated poor prognosis remains poor even after taking into account CD4 levels.
The underlying mechanism for cardiomyopathy and left ventricular dysfunction in HIV/AIDS remains incompletely understood.
Suggestions of possible mechanisms include:
Pathologies due to HIV and HIV-associated proteins
Cytokines
Lymphocytic myocarditis
Autoimmune response abnormalities
Drugs,
Suboptimal nutrition et al.9
Other Cardiovascular Dysfunctions Described in HIV Patients2
In patients with HIV infection other cardiovascular dysfunctions in addition to those previously described may also be present.2
Advanced HIV disease may cause pericardial effusions.2
|
|
|
|
|
|
Factors that may increase the likelihood of pericardial effusion include:
Tuberculosis
Congestive heart failure
Cryptococcal or myobacterial infection
Pulmonary infection
Kaposi's sarcoma
Lymphoma.
Pericardial Kaposi's sarcoma may be associated with both tamponade and death, probably due to acute hemorrhage.
Occasionally, nonbacterial thrombotic endocarditis may occur.
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |