|
|
|
|
|
|
|
Nursing Pharmacology: Antiviral Drugs
|
|
|
|
|
|
|
Antiviral Drugs
Anti-viral drugs with activity against HIV (Human Immunodeficiency Virus)
HIV-1 Pathophysiology/Pathogenesis: HIV Disease Presentations
|
|
|
HIV patients may be affected by gallbladder and biliary diseases.9
Some of these disorders are quite common such as non-HIV-associated cholelithiasis (lithiasis (stone fomration) in the galbladder)
|
|
|
Common AIDS-associated conditions include acalculous cholecystitis and cholangiopathy.9
Such patients may exhibit postprandial discomfort (pain), fever, upper right quadrant pain and tenderness as well as elevated serum alkaline phosphatase.
Either ultrasonography or computed tomography (CT) imaging may reveal acute cholecystitis or cholangitis related to cholelithiasis.9
 |
|
In patients with advanced HIV disease, such findings may indicate acalculous cholecystitis or AIDS-associated cholangitis.9,10
Should a cholecystectomy be performed in an HIV patient, specimens from the gallbladder should be sent to pathology for evaluation.11
Prior to the availability of cART (HAART) combined highly active antiretroviral drugs, opportunistic pathogens were found in the following study in >50% of cases.11
This clinical study that described these opportunistic pathogens in HIV patients was based on such patients undergoing cholecystectomy between February 1987 and May 1993.
Pathogens described in this study of 107 AIDS patients included microsporidia (Enterocytozoon bienuesi and Septata intestinalis), Cryptosporidium, cytomegalovirus + Cryptosporidium, Pneumocystis jiroveci (PCP) and Isospora belli.11
Histologic changes consistent with Kaposi's sarcoma was also noted in one case.
In 38 AIDS patients with acalculous cholecystitis, no etiologic agent was determined.
Furthermore, 28 AIDS patients had cholelithiasis and some exhibited coexistent opportunistic gallbladder infection.11
If cART combination anti-retroviral treatment is being administered the likelihood of AIDS cholangiopathy appears quite low, suggesting that this disorder might be seen in patients with CD4+ T cell counts of <50mm3.9
In the cART setting, noninfectious disease such as cholelithiasis likely accounts for the increased proportion of hepatobiliary disease in HIV patients.
One HIV protease inhibitor, atazanavir, may predispose the patient to biliary stone development and the stones are found to contain "significant concentration of the actual drug."9
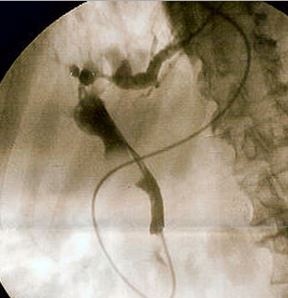
![]() Under
the circumstances in which noninvasive radiographic imaging studies
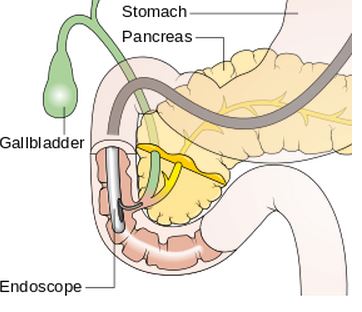
suggest intrahepatic/extrahepatic biliary ductal dilation, ERCP (endoscopic
retrograde cholangiopancreatography) may be required for diagnosis
and optimal management of AIDS-associated cholangiopathy.9
Under
the circumstances in which noninvasive radiographic imaging studies
suggest intrahepatic/extrahepatic biliary ductal dilation, ERCP (endoscopic
retrograde cholangiopancreatography) may be required for diagnosis
and optimal management of AIDS-associated cholangiopathy.9
|
|
|
|
![]() Four
distinctive patterns describing cholangiographic pathologies may be
noted with ERCP.9
Four
distinctive patterns describing cholangiographic pathologies may be
noted with ERCP.9
These patterns include:
Papilla of Vater stenosis with associated dilated extrahepatic biliary tract
Sclerosing cholangitis
Sclerosing cholangitis + papillary stenosis
Choledochal long stenosis/strictures9
Opportunistic pathogens or malignant diseases may be determined from endoscopic bile collection from the common bile duct along with duodenal or papillary biopsy.9
Cholangitis (similar to acalculous cholecystitis noted earlier) occurs with opportunistic infections > 50% of cases.
These infections include:
CMV (cytomegalovirus)
Cryptosporidium
Microsporidia 9
Additional infectious pathogens that have been identified include Cryptococcus neoformans, Cystoisospora belli, and pneumocystis jiroveci.9
Biliary tree malignancies that have been described include lymphoma and Kaposi's sarcoma.9
In one study undertaken as a result of a 1993 municipal water supply in Milwaukee, Wisconsin (USA) Cryptosporidia contamination with a resulting cryptosporidosis outbreak.15
The authors evaluated retrospectively associations among clinical presentation, CD4+ T cell count, and survival in a group of 82 patients who had been infected with HIV and who developed cryptosporidosis during this outbreak.
A clear increase in the number of HIV-infected patients with cryptosporidosis was noted following the period of water contamination.
Some patients (four of 24) displayed biliary symptoms; however, 30 of 58 presented without biliary symptoms.15
4 of the 24 and 30 of the 58 remained alive one year following the outbreak. 21 patients (80%) with biliary symptoms exhibited CD4+ T cell counts ≤ 50/mm3. 36 of 57 (63%) without biliary symptoms had CD4+ T cell counts ≤ 50/mm3.
![]() The
clinical study suggested that when HIV-infected
patients are exposed to Cryptosporidium, and
have CD4+ T cell counts
≤
50/mm3,
both an increased risk for biliary symptoms and
death are found within one year after infection.15
The
clinical study suggested that when HIV-infected
patients are exposed to Cryptosporidium, and
have CD4+ T cell counts
≤
50/mm3,
both an increased risk for biliary symptoms and
death are found within one year after infection.15
 |
|
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |


_CRUK_001.svg){kind=link}
{kind=link}