|
|
|
|
|
|
|
Nursing Pharmacology: Antiviral Drugs
|
|
|
|
|
|
|
Antiviral Drugs
Anti-viral drugs with activity against HIV (Human Immunodeficiency Virus)
HIV-1 Pathophysiology/Pathogenesis: HIV Disease Presentations
Acute Kidney Injury (AKI)5
![]() Factors
resulting in acute kidney injury (AKI) noted in patients who are HIV
negative are also seen in the HIV-infected population.5
Factors
resulting in acute kidney injury (AKI) noted in patients who are HIV
negative are also seen in the HIV-infected population.5
![]() For
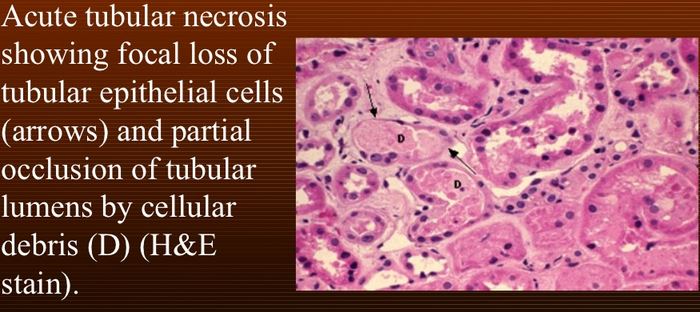
example volume depletion, hypotension, or sepsis can cause acute
tubular necrosis and prerenal azotemia.5
For
example volume depletion, hypotension, or sepsis can cause acute
tubular necrosis and prerenal azotemia.5
Acute tubular necrosis damages the renal tubule cells and is a common cause of kidney failure in hospitalized patients.6
 |
|
Opportunistic infections may be treated by nephrotoxic drugs.
![]() Opportunistic
infections themselves such as cytomegalovirus (CMV), candida,
tuberculosis, histoplasmosis as well as a variety of drugs can
result in interstitial nephritis.
Opportunistic
infections themselves such as cytomegalovirus (CMV), candida,
tuberculosis, histoplasmosis as well as a variety of drugs can
result in interstitial nephritis.
CMV-related pathologies can include nephrocalcinosis.
![]() Sometimes
renal disease may be the presenting indication of HIV
infection.
Sometimes
renal disease may be the presenting indication of HIV
infection.
Thrombotic thrombocytopenic purpura and hemolytic uremic syndrome is such an example.
Some drugs including acyclovir, atazanavir, indinavir, and sulfadiazine administration may result in crystal-induced obstructive acute kidney injury.5
Indinavir appears associated with asymptomatic crystalluria in as many as 20% of individuals.
In hospitalized HIV-infected individuals electrolyte abnormalities may be frequently encountered.5
For example, up to 30%-50% of hospitalized AIDS patients exhibit hyponatremia.
Up to 20% of hospitalized AIDS patients may exhibit elevated serum potassium i.e. hyperkalemia.
Effects on electrolytes may follow from not only direct consequences of HIV infection but also from opportunistic infections along with drugs used to manage such infections including combination anti-retroviral (cART anti-HIV) medications.
Relationships between abnormal electrolytes and mechanisms in HIV-infected individuals have been described.5
Hyponatremia (low serum sodium)5
Volume depletion
SIADH (Syndrome of inappropriate antidiuretic hormone secretion (Schwartz-Bartter syndrome), secondary to CNS and pulmonary dysfunction.
Adrenal insufficiency: reduced or absolute adrenal glucocorticoid and/or mineralocorticoid hormones9
Hypernatremia5
Volume depletion (reduced oral intake)
Acquired nephrogenic diabetes insipidus (medication-induced)
|
Hyperkalemia5
Hyperkalemia may occur as a consequence of drug administration.
Examples of drugs with this effect possibly seen in the HIV-infected population include:
Pentamidine
Trimethoprim
Hyporeninemic hypoaldosteronism may also be associated with elevation in K+.5
This disorder may also be described as type IV renal tubular acidosis.16
Hyperkalemia and acidosis present along with typically mild chronic renal disease.
The pathophysiology is likely due to reduced renin production by the juxtaglomerular apparatus along with underlying renal pathology.
However, the chronic kidney disease component is typically insufficient to account for the observed hyperkalemia.
![]() Reduced
secretion of both K+ and H+ in the renal tubule
appears responsible for the noted hyperkalemia and metabolic acidosis.16
Reduced
secretion of both K+ and H+ in the renal tubule
appears responsible for the noted hyperkalemia and metabolic acidosis.16
Adrenal insufficiency is another potential cause of hyperkalemia.5
Adrenal insufficiency in HIV-infected patients is typically associated with advanced disease.16
Opportunistic infections that target the adrenal gland include:
Cytomegalovirus (CMV)
Disseminated Mycobacterium avium-intracellulare
M tuberculosis
Cryptococcus neoformans
Pneumocystis jiroveci (PCP) as well as
Toxoplasma gondii
The adrenal gland may also be affected by neoplasms such as Kaposi's sarcoma.16
Clinical adrenal insufficiency is generally uncommon.16
However, more than 50% of individuals with AIDS exhibit necrotizing adrenalitis usually from cytomegalovirus infection.
Necrotizing adrenalitis in this setting affects less than about 50%-70% of the adrenal gland; however, adrenal insufficiency requires typically greater than 90% gland destruction.
Steroid secretion and metabolism can be altered by medications including ketoconazole which inhibits adrenal and gonadal steroid synthesis.
By contrast, rifampin, phenytoin and opioids enhance steroid metabolism.16
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |