|
|
|
|
|
|
|
Nursing Pharmacology: Antiviral Drugs
|
|
|
|
|
|
|
Non-nucleoside/Nucleotide Reverse Transcriptase Inhibtors (NNRTI)
Antiretroviral Drugs Used in Treating HIV Infection
→Non-nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NNRTI): Introduction
|
|
|
|
|
|
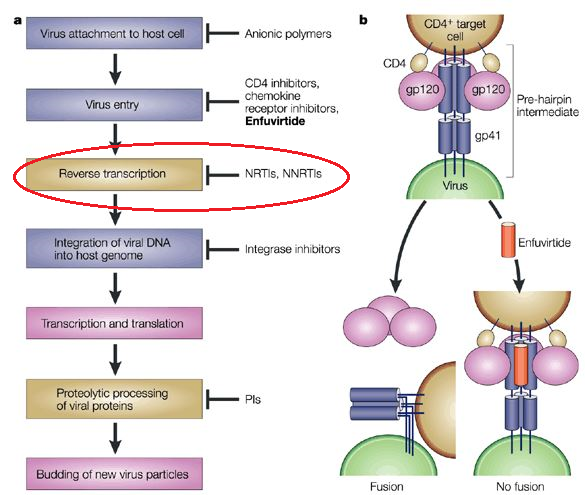
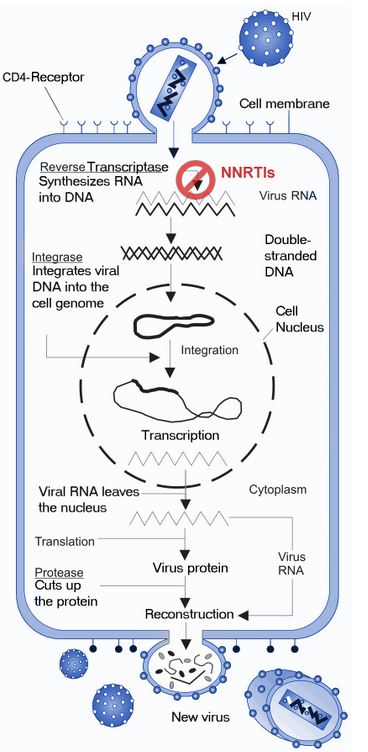
Non-nucleoside reverse transcriptase inhibitors are classified as noncompetitive, acting by inducing a conformational change in the enzyme as opposed to competing with other molecules at the binding site (competitive inhibition).1
Binding site specificity for these drugs results in their activity against HIV-1 but these agents are not active against HIV-2 or other retroviruses.
Furthermore the non-nucleoside reverse transcriptase inhibitors did not exhibit activity with respect to cell DNA polymerases.1
Efavirenz and nevirapine are examples of drugs in this category and represents the two agents most frequently administered.1
Employed as monotherapy, administration of these drugs may decrease in HIV RNA plasma concentrations by a factor of 100 or more, although resistance typically rapidly develops.13
Non-nucleoside reverse transcriptase inhibitors (presently approved) utilize the liver microsomal metabolizing system for elimination.1
The cytochrome P450-dependent system describes a variety of cytochrome P450 similar enzymes or "isoforms".
For example, delavirdine and nevirapine are primarily metabolized by an important drug metabolizing isoform, CYP3A4.
By contrast, efavirenz is mainly metabolized by CYP2B6 and CYP3A4.
Elimination half-times for efavirenz and nevirapine extend from 1 to 3 days which permits daily dosing.
Sometimes drugs are also able to induce cytochrome P450 enzymes, resulting usually and elevated enzyme cellular concentrations.
![]() In this
instance, efavirenz, etravirine, and nevirapine are
classified as moderately potent inducers of the cytochrom P450 system.1
In this
instance, efavirenz, etravirine, and nevirapine are
classified as moderately potent inducers of the cytochrom P450 system.1
In particular, these agents elevate CYP3A4 levels; however, delavirdine has been shown to be a CYP3A4 inhibitor.
A further complication is that a drug may inhibit some cytochrome P450 isoforms while inducing others.
This effect, "mix metabolism", describes the case noted for etravirine.1
![]() Changes
in concentrations or activities of cytochrome P450 isoforms may result
in drug-drug interactions.1
Changes
in concentrations or activities of cytochrome P450 isoforms may result
in drug-drug interactions.1
For example, if one drug increases the concentration of the cytochrome P450 isoform mainly responsible for the metabolism of the second drug, the plasma concentration of the second drug may decrease to below therapeutic levels.
Should one drug decrease the concentration of a cytochrome P450 isoform which metabolizes a second drug, plasma concentration of the second drug may be increased resulting in toxicities.
Microsomes have been used to study mixed function oxidases
Drug metabolizing enzymes are located in lipophilic, hepatic endoplasmic reticulum membranes. Smooth endoplasmic reticulum contains those enzymes responsible for drug metabolism.
![]() Currently,
FDA-approved non-nucleoside reverse transcriptase inhibitors include:9
Currently,
FDA-approved non-nucleoside reverse transcriptase inhibitors include:9
Delavirdine (DLV)
Efavirenz (EFV)
Etravirine (ETR)
Nevirapine (NVP) and
Rilpivirine (RPV).
Genotypic testing is suggested prior to initiating NNRTI treatment because of relatively high resistance rate: 2%-8%.7
NNRTI resistance, as noted, develops quickly with monotherapy and may occur following a single mutation.7
Examples of mutations include K103N, a substitution of lysine by asparagine, noted in resistance to nevirapine and Y181C, a substitution of a tyrosine by a cysteine.
These mutations appear more likely to induce resistance to the first-generation NNRTI agents while not affecting newer drugs such as rilpivirine and etravirine.
Some mutations induce cross-resistance to drugs belonging to the NNRTI drug group.7
With the exception of etravirine, other NNRTI agents may exhibit significant drug resistance due to single-amino-acid substitutions in the drug-binding allosteric region.1
![]() By
contrast, other HIV-1 antiretroviral drugs belonging to the
nucleoside analog or protease inhibitor classes, efavirenz or
nevirapine resistance and associated virologic relapse may occur
quickly, within a few days or weeks, if the drug is administered as
monotherapy.
By
contrast, other HIV-1 antiretroviral drugs belonging to the
nucleoside analog or protease inhibitor classes, efavirenz or
nevirapine resistance and associated virologic relapse may occur
quickly, within a few days or weeks, if the drug is administered as
monotherapy.
![]() As monotherapy, a single dose of nevirapine may be associated
with mutations resulting in drug resistance in as many as 33% of
patients.1
As monotherapy, a single dose of nevirapine may be associated
with mutations resulting in drug resistance in as many as 33% of
patients.1
![]() As a
result of these considerations, NNRTI antiretroviral drugs must be
administered in combination with a minimum of two other active drugs
in order to avoid drug resistance.1
As a
result of these considerations, NNRTI antiretroviral drugs must be
administered in combination with a minimum of two other active drugs
in order to avoid drug resistance.1
Efavirenz or nevirapine administration along with other antiretroviral agents results in long-term suppression of viremia and increases in CD4+ T lymphocyte counts.1
Efavirenz is frequently used as a component of the first drug regimen in treatment-naïve patients.
Efavirenz is favored in this setting as a result of convenience of use, patient's ability to tolerate the drug, and drug potency.
A common side effect associated with NNRTIs, most likely occurring within the first month of treatment is a mild, self-limited rash.
Rare cases of potentially fatal Stevens-Johnson syndrome have been documented with nevirapine, efavirenz, and etravirine.1
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |