|
|
|
|
|
|
|
Nursing Pharmacology : Antiviral Drugs
|
|
|
|
|
|
|
Antiretroviral Drugs Used in Treating HIV Infection
→Integrase Strand Transfer Inhibitors (INSTI):
By way of review, HIV-1 replication depends on three enzymes: viral reverse transcriptase, protease and viral integrase.18
Following interaction with host cells expressing surface CD4+ receptors and required co-receptors, HIV enters the cell and its single-stranded RNA genome is converted into a double-stranded form viral reverse transcriptase.
Integration of HIV-1 complementary DNA (complementary to the original HIV-1 RNA), utilizes HIV-1 integrase in promoting a two-step process.
(1) The first step involves excision of two nucleotides from the 3' ends of HIV-1 DNA.
(2) Subsequently, covalent insertion of HIV-1 viral genomic DNA into the host cell chromosome occurs.
![]() Inhibition of the integrase
enzyme results in viral complementary DNA circularization, a process
catalyzed by host cell enzymes, as well as nuclear accumulation of 2-long
terminal repeat (LTR) circles.
Inhibition of the integrase
enzyme results in viral complementary DNA circularization, a process
catalyzed by host cell enzymes, as well as nuclear accumulation of 2-long
terminal repeat (LTR) circles.
Stable integration of HIV-1 DNA into the host genome is therefore prevented by inhibition of viral integrase.
Consequently, viral latency within the host cell allowing HIV-1 replication and elaboration new virus is prevented.18
|
Dolutegravir (Tivicay) |
Dolutegravir is the most recent and third example of a strand transfer integrase inhibitor drug for use in treating HIV-1 infection.15
|
|
|
By contrast to elvitegravir, no boosting agent is required.
A single dose (50 mg/day) may be appropriate in treatment-naïve/integrase drug-naïve individuals.
Those patients receiving efavirenz, tipranavir + ritonavir combination treatment, fosamprenavir + ritonavir combination or rifampin may require two 50 mg doses of dolutegravir per day.
![]() This higher
dosage may also be appropriate in patients previously treated within
integrase-inhibitor and in whom possible resistance to integrase
inhibitors may be occurring.15
This higher
dosage may also be appropriate in patients previously treated within
integrase-inhibitor and in whom possible resistance to integrase
inhibitors may be occurring.15
Dolutegravir (Tivicay) in the unboosted form is a recent example of an integrase strand transfer inhibitor, exhibiting extended plasma half-life (≈14 hours), thus allowing for once a day dosing absent a requirement for pharmacokinetic boosting.12
In August 2013 dolutegravir received FDA approval and later that year, in November 2013 dolutegravir was approved by Health Canada. In early 2014 dolutegravir (Tivicay) was approved by the European Commission for use throughout the European Union.
Although dolutegravir is being evaluated for combination therapy with abacavir and lamivudine12, dolutegravir has been shown to exhibit potent antiviral activity with good short-term tolerability.11,12
![]() Based on
clinical trials involving treatment-naïve HIV-infected individuals, results
with dolutegravir have been considered "impressive" when compared with, for
example, nonnucleoside reverse transcriptase inhibitors (NNRTI, boosted
protease inhibitors (PI) and raltegravir-containing protocols.
Based on
clinical trials involving treatment-naïve HIV-infected individuals, results
with dolutegravir have been considered "impressive" when compared with, for
example, nonnucleoside reverse transcriptase inhibitors (NNRTI, boosted
protease inhibitors (PI) and raltegravir-containing protocols.
Furthermore, dolutegravir was found superior both to the combination treatment efavirenz + tenofovir + emtricitabine and to the protocol consisting of darunavir (Prezista) + ritonavir + tenofovir + emtricitabine in those patients who exhibited baseline HIV viral RNA loads >100,000 copies/mL.
Mutations and Resistance to Dolutegravir:
Many of the prominent mutations associated with the integrase strand inhibitor agents reduce dolutegravir sensitivity.6
![]() However, if
more than two integrase strand inhibitor-resistance mutations was initially
present, virologic failure ensued.
However, if
more than two integrase strand inhibitor-resistance mutations was initially
present, virologic failure ensued.
As noted earlier, dolutegravir exhibits a half-life of ≈ 14 hours.6
Dolutegravir is metabolized principally by phase II glucuronidation (catalyzed by the UGT1A1 gene product, a glucuronosyltransferase1) and with minor oxidative pathways catalyzed by the cytochrome P450 isoform CYP3A4 (8% of parent compound).7,17
Given that dolutegravir is metabolized by both phase I and phase II (i.e. UGT1A1-coded glucuronosyltransferase and cytochrome P450 (i.e. CYP3A4), drug-drug interactions may be expected.7
For example, administration of dolutegravir with inducers of these metabolizing enzymes such as phenobarbital, carbamazepine, phenytoin, and St. John's wort may be inappropriate.
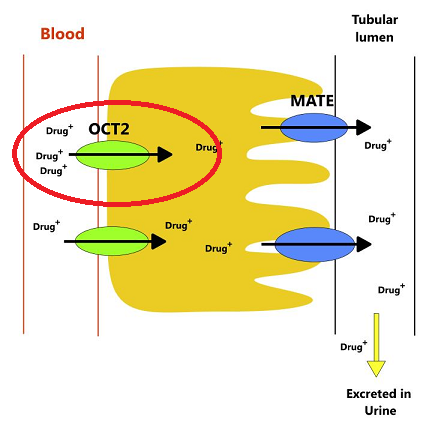
Another characteristic of dolutegravir is inhibition of an important organic anion transporter, OCT2, found in the kidney.
|
|
|
Inhibition of this transporter may increase plasma concentration of drugs dependent on OCT2 including metformin.7
This transporter, OCT2 (Organic Cation Transporter 2) is expressed in the three segments of human renal proximal tubules as well is in small intestine.
OCT2 is localized in epithelial cell basolateral membranes as well as epithelial luminal membranes of trachea and bronchi.
However it is most prominently expressed in the kidney, although also expressed in lung, skin, brain, choroid plexus and placenta.19-23
Insomnia and headache represent the most common adverse reactions to dolutegravir administration.7
![]() Other
reactions including hypersensitivity associated with rash and even organ
dysfunction including hepatic damage have been described and could be
life-threatening. Immediate cessation of drug administration without
subsequent re-administration would be appropriate should such
hypersensitivity reaction ensue.
Other
reactions including hypersensitivity associated with rash and even organ
dysfunction including hepatic damage have been described and could be
life-threatening. Immediate cessation of drug administration without
subsequent re-administration would be appropriate should such
hypersensitivity reaction ensue.
"Fat redistribution" syndrome along with increases in serum aminotransferase enzyme levels have also been reported.7
A recommended INSTI-based protocol for HIV treatment in treatment-naïve patients is based on dolutegravir combination with abacavir and lamivudine (DTG/ABC/3TC) ONLY in HLA-B*5701 negative individuals.9
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |