|
|
|
Nursing Pharmacology: Antiviral Drugs
|
|
|
Antiretroviral Drugs Used in Treating HIV Infection
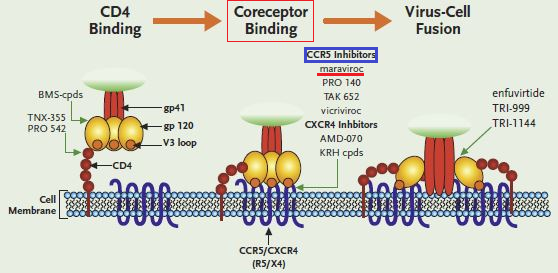
→Entry Inhibitors: The drug enfuvirtide, derived from gp41, binds to gp41 in a way that prevents the structural change needed for fusion (see previous page).
![]() Another drug, maraviroc, inhibits
viral entry by binding to one of the chemokine HIV co-receptors, CCR5, thus
inhibiting interaction with gp120 and inhibiting fusion initiation.1
Another drug, maraviroc, inhibits
viral entry by binding to one of the chemokine HIV co-receptors, CCR5, thus
inhibiting interaction with gp120 and inhibiting fusion initiation.1
In 2007 the US FDA approved the first member of a new group of antiretroviral drugs used for treating HIV-1 infection.2
This agent, Maraviroc (Selzentry, Celsentri) acts by interfering with the interaction between HIV-1 gp120 protein and the chemokine co-receptor CCR5.
Maraviroc was FDA approved for use in those patients experiencing virologic failure secondary to resistance to other antiviral medications.2
|
|
|
Studies about 30 years ago identified the CD4 receptor as the principal target for HIV-1 binding to CD4+ cells.
Experiments using hybrid mouse cells expressing human CD4+ indicated that CD4+ binding by itself is insufficient to cause viral entry.
Subsequently, two co-receptors were discovered.
These co-receptors were CCR5 (C-C chemokine Receptor type 5)and CXCR4 and were chemokine receptors which were also necessary for viral entry, along with the CD4+ receptor.
CCR5 is associated with naturally occurring ligands:
These HIV-1 co-receptors, CXCR4 and CCR5, are part of the G protein-coupled receptor superfamily described in earlier sections.6
CCR5 is considered an especially important therapeutic target since genetic absence of surface expression of this protein confers nearly complete resistance to HIV-1 infection.7
Maraviroc (Selzentry, Celsentri) Pharmacology
Introduction:
Maraviroc inhibits association between gp120, HIV outer envelope protein, and the CCR5 chemokine receptor.8
Maraviroc activity is limited to those HIV strains expressing CCR5 and therefore exhibits no activity against those HIV strains which are either CXCR4 expressing or which express both CCR5 and CXCR4 co-receptors.
As a result of this focused mechanism of action, Maraviroc has the advantage of retaining antiretroviral efficacy even when HIV strains exhibit resistance to other antiretroviral drugs.8
Drug Resistance:2
Resistance to the antiretroviral activity of Maraviroc appears to occur in either of two mechanisms.2
The first mechanism involves a change in tropism such that the HIV-1 strain becomes able to use the CXCR4 chemokine co-receptor.
The second mechanism allows HIV-1 to continue to use the CCR5 co-receptor even though it is being blocked by Maraviroc.
![]() Of
these two mechanisms of resistance development,
the change in tropism may be of particular
clinical concern since virus that can use the
CXCR4 co-receptor may be associated with a more
rapid decline in CD4+ lymphocyte
count and disease progression.10
Of
these two mechanisms of resistance development,
the change in tropism may be of particular
clinical concern since virus that can use the
CXCR4 co-receptor may be associated with a more
rapid decline in CD4+ lymphocyte
count and disease progression.10
However, the main mechanism of Maraviroc resistance is likely the ability of HIV-1 to use Maraviroc-associated CCR5 co-receptors.
In this setting increasing concentrations of Maraviroc does not result in increased viral inhibition. Intrinsic resistance to Maraviroc appears limited and cross-resistance with the fusion inhibitor enfuvirtide has not been observed.2
Pharmacokinetics:9
The dose-dependent oral bioavailability of Maraviroc is about 20%-30%.
Food decreases bioavailability as much as 50% in this agent exhibits protein binding in human plasma in the range of about 75%.
The P450 microsomal metabolizing system is responsible for biotransformation and supports Maraviroc elimination with a half-life of about 10 hours.
The P450 isozyme primarily implicated in elimination is CYP3A4.2
![]() Pharmakokinetics
of Maraviroc may be affected by agents that inhibit
CYP3A.
Pharmakokinetics
of Maraviroc may be affected by agents that inhibit
CYP3A.
![]() For example, itraconozole,
lopinavir, lopinavir plus ratonavir, ratonavir,
saquinavir and ataznavir increase maximal plasma
concentration of Maraviroc as well as increasing the
area under the curve (AUC).2
For example, itraconozole,
lopinavir, lopinavir plus ratonavir, ratonavir,
saquinavir and ataznavir increase maximal plasma
concentration of Maraviroc as well as increasing the
area under the curve (AUC).2
Clinical/Therapeutic Uses:9
Maraviroc (Selzentry, Celsentri) is FDA approved for use in HIV-infected patients (adults) whose HIV infection consists mainly of the CCR5-tropic virus.
![]() The
addition of Maraviroc to patients receiving optimal,
typically multidrug antiviral treatment but with
documented multidrug resistant HIV-1 appears clinically
beneficial.
The
addition of Maraviroc to patients receiving optimal,
typically multidrug antiviral treatment but with
documented multidrug resistant HIV-1 appears clinically
beneficial.
|
|
|
Noting that Maraviroc adminstration results in limited to no therapeutic effectiveness in those patients whose HIV-1 strain exhibits CXCR4 or dual/mixed CCR5 + CXCR4 chemokine co-receptors, Maraviroc cost-effectiveness may be limited due to the need for phenotype testing.9
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |