Nursing Pharmacology Chapter 11: Drugs Used in Treating Hyperlipidemia
|
|
|
|
|
|
|
Overview: lipoprotein disorders
Evaluation: Serum lipid measurement following 10-hour fast
CHD risk:
Directly proportional to atherogenic lipoproteins concentration
Indirectly proportional to HDL levels
Triglyceride levels, preferably less than 150 mg/dL
|
Definition: triglyceride plasma concentration > 90th or 95th percentile for age and gender (as determined following an overnight fast)
Isolated plasma triglycerides elevation may be due to increased VLDL or combinations of elevated VLDL and chylomicrons (rarely a result of elevated chylomicrons only)
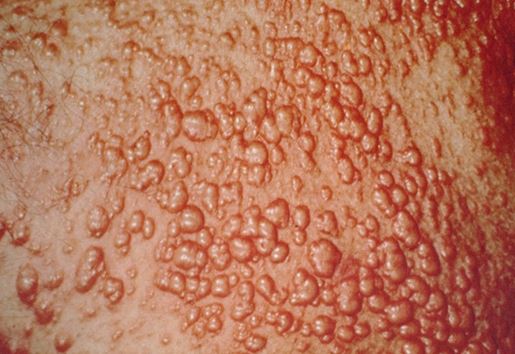
Eruptive xanthomas may occur in isolated hypertriglyceridemia
Small, orange-red papules (trunk/extremities; triglyceride levels > 1000 mg/dL chylomicronemia)
|
|
|
at 1000 mg/dL:
Orange-yellow retinal vessels (lipemia retinalis)
Major risk at this plasma triglyceride concentration: pancreatitis
Regulation of hepatic triglyceride synthesis:
Free fatty acid availability
Hepatic glycogen levels
Balance between insulin and glucagon
![]() Conditions associated
with hypertriglyceridemia:
Conditions associated
with hypertriglyceridemia:
Obesity, insulin resistance, alcohol consumption, inactivity, excessive intake of simple sugars and saturated fats.
At VLDL triglyceride levels > 1000 mg/dL, lipoprotein lipases may become saturated
![]() Familial
Hypertriglyceridemia: (severe)
Familial
Hypertriglyceridemia: (severe)
Autosomal dominant (For mixed lipemia there are various modes of inheritance)
Possible mechanisms: VLDL overproduction and reduced triglyceride-rich lipoprotein catabolism
Fasting triglyceride range: 200-750 mg/dL, with increased VLDL triglycerides only
Factors that increase VLDL production worsens lipemia (VLDL and chylomicrons which are competing lipoprotein lipase substrates)
Most patients: obese
Clinical complaints (depending on lipemia severity): eruptive xanthomas, epigastric pain, lipemia retinalis, pancreatitis
Treatment: dietary -- alcohol avoidance, reduced fat intake, avoid exogenous estrogen, weight reduction; some patients may benefit from gemfibrozil (Lopid) or niacin (vitamin B3)
![]() Familial
Hypertriglyceridemia:
(moderate, endogenous lipemia)
Familial
Hypertriglyceridemia:
(moderate, endogenous lipemia)
Multiple genetic factors
Made worse by factors that increased hepatic VLDL secretion (hypertrophic obesity, alcohol, exogenous estrogen intake, diabetes)
Treatment: -- indication presence of atherosclerosis (in the patient or in the patient's family)
Weight reduction
Dietary fat restriction
Alcohol avoidance
If necessary, gemfibrozil (Lopid) or niacin (vitamin B3)
![]() Familial Combined
Hyperlipoproteinemia:
Familial Combined
Hyperlipoproteinemia:
Elevated VLDL and/or LDL
Mechanism: 200% increase in hepatic VLDL secretion
Increased CHD risk: Drug therapy (niacin or a resin in combination with niacin)
![]() Familial Lipoprotein Lipase
Deficiency:
Familial Lipoprotein Lipase
Deficiency:
Autosomal recessive (absence/impairment of lipoprotein lipase/lipoprotein lipase cofactor)
Dramatic chylomicron accumulation in plasma:
Lipemia worsened by estrogens and pregnancy
![]() Clinical presentations
(beginning in infancy) include:
Clinical presentations
(beginning in infancy) include:
Pancreatitis
Eruptive xanthomas
Hepatomegaly
Splenomegaly
Bone marrow foam cell infiltration
At triglyceride levels > 1000 mg/dL --lipemia retinalis
Familial Apoprotein CII Deficiency:
Rare autosomal recessive
Presentations similar to familial lipoprotein lipase deficiency
Familial Dysbetalipoproteinemia:
Accumulation of chylomicrons and VLDL reminants
Low LDL; high serum cholesterol and triglycerides
Clinical Presentations:Familial Dysbetalipoproteinemia:
Tuberous/tuberoeruptive xanthomas
Planar xanthomas:palmar creases
Common: obesity and impaired glucose tolerance-- worsening lipemia
Peripheral/coronary atherosclerosis
Treatment: Familial Dysbetalipoproteinemia:
Weight reduction
Reduced fat, cholesterol, alcohol intake
Niacin (vitamin B3) or gemfibrozil (Lopid) may be needed (typically at low doses).
Primary Reference: Malloy, M. J, and Kane, J. P., Agents Used in Hyperlipidemia, in Basic and Clinical Pharmacology, (Katzung, B. G., ed) Appleton-Lange, 1998, pp 563-577.
Primary Reference: Ginsberg, H. N and Goldberg, I. J. Disorders of Intermediary Metabolism: Disorders of Lipoprotein Metabolism, In Harrison's Principles of Internal Medicine 14th edition, (Isselbacher, K.J., Braunwald, E., Wilson, J.D., Martin, J.B., Fauci, A.S. and Kasper, D.L., eds) McGraw-Hill, Inc (Health Professions Division), 1998, pp 2138-2149.
|
|
|
|
|
|
|