|
|
|
|
|
|
|
Nursing Pharmacology Chapter 33-34: Anticancer Drugs
|
|
|
|
|
|
|
Hormonal Anticancer Drugs:
Cancer cell proliferation is influenced by hormones, with proliferation either regulated or hormonal dependent.1
Glucocorticoids administration may reduce neoplastic cell proliferation as well as exhibit lympholytic (lymphocyte cell death promoting) properties.
Anticancer effects are associated with administration of:
Estrogen inhibitors
Androgen inhibitors
Steroid synthesis inhibitors
Gonadotropin-releasing hormone (GnRH) analogues or inhibitors.1
Sometimes administration of these agents prolong survival and can delay or prevent tumor recurrence, for example in prostate cancer and breast cancer.
|
Modes of action of these agents include:1
Interference with a "stimulatory axis" due to systemic androgens and estrogens
Hormone production inhibition
Inhibition of hormone-receptor association
Inhibition of gene expressions that enhance cancerous tumor growth.1
Hormonal-based treatments are also used in managing "paraneoplastic syndromes" for example, carcinoid syndrome as well as cancer-caused symptoms such as anorexia.3
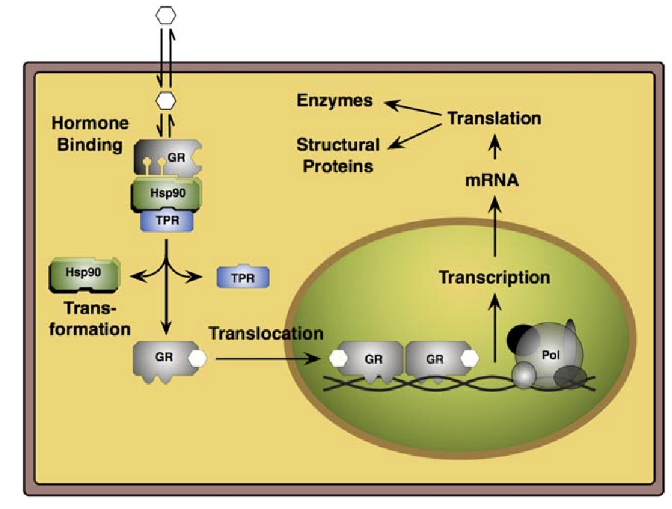
![]() Glucocorticoids exert their pharmacological properties as a result of
binding to a particular glucocorticoid receptor (GR or GCR) .1,9
Glucocorticoids exert their pharmacological properties as a result of
binding to a particular glucocorticoid receptor (GR or GCR) .1,9
![]() This receptor
belongs to a group of nuclear receptors that regulate transcription factors.
This receptor
belongs to a group of nuclear receptors that regulate transcription factors.
Other members of the "nuclear hormone receptor superfamily" in addition to the estrogen receptor include:2
Progesterone receptor (PR)
Androgen receptor (AR)
Glucocorticoid receptor (GR)
Mineralocorticoid receptor.
This receptor grouping, moreover, also includes nonsteroidal nuclear hormone receptors including:
Retinoids
Vitamin D (deltanoids)
Thyroid hormones.2
Following glucocorticoid binding in the cytosol, the glucocorticoid receptor-glucocorticoid comples relocates to the cell nucleus, where the complex induces changes in gene expression.
|
|
|
![]() These
changes in sensitive cells promote apoptosis and anti-cell division
responses (antiproliferative).
These
changes in sensitive cells promote apoptosis and anti-cell division
responses (antiproliferative).
Anti-proliferative responses manifest in reduced lymphocyte mitosis.
Furthermore, lympholytic effects are also prominent.
![]() Because
of these actions, glucocorticoids are effective in treating
childhood acute leukemia and malignant lymphoma in both
children and adults.
Because
of these actions, glucocorticoids are effective in treating
childhood acute leukemia and malignant lymphoma in both
children and adults.
Glucocorticoid administration, used to treat lymphoblastic or undifferentiated childhood leukemia, may result in rapid clinical improvement.
Hematological remissions are described in about 1/3 of pediatric patients.
Unfortunately, remission duration may be brief and may occur earlier with glucocorticoids compared to anti-metabolite antineoplastic drugs.
As a result, initial treatment may involve both prednisone and vincristine with subsequent treatment with an anthracycline drug or methotrexate and L-asparaginase.1
High-dose estrogen administration is an effective agent for treating breast cancer.1
Antineoplastic effects of estrogen may be associated with drug -induced apoptosis noted in endocrine-resistant disease.
Estrogen signaling may also be inhibited by antiestrogens.
![]() A prominent
antiestrogen is tamoxifen.
A prominent
antiestrogen is tamoxifen.
Other ways of interfering with estrogen -related signaling is by direct reduction of estrogen synthesis by agents classified as aromatase inhibitors (AI) and gonadotropin-releasing hormone (GnRH) structural analogs.
![]() These
analogs have advantages in terms of both effectiveness and patient
tolerance.
These
analogs have advantages in terms of both effectiveness and patient
tolerance.
Furthermore, these agents have superseded estrogens or androgens for breast cancer management.
The presence of estrogen receptor (ER) and progesterone receptor (PR) on neoplastic breast cancer cells increase the likelihood of hormonal therapy response.
![]() Breast
cancer tumors that are positive (expressing) ER+ or positive
(expressing) PR+ and also exhibit human epidermal growth factor
receptor HER2/neu amplification show somewhat lower response to antiestrogen
protocols.
Breast
cancer tumors that are positive (expressing) ER+ or positive
(expressing) PR+ and also exhibit human epidermal growth factor
receptor HER2/neu amplification show somewhat lower response to antiestrogen
protocols.
Breast cancers not expressing ER or PR are not responsive to hormonal treatment.1
![]() Estrogen and Related
Agents: Structures:
Estrogen and Related
Agents: Structures:
There are three endogenous, naturally occurring estrogens:
Estradiol
Estrone
Estriol.
The structures are produced by testosterone and anthracenedione aromatization (respectively)
|
|
|
|
|
|
|