|
|
Medical Pharmacology Chapter 48: Assessment of Pulmonary Function in Normal and Pathological States: An Introduction
|
|
1The two classifications for ventilation defects are "restrictive" and "obstructive".
Patients may have both restrictive than obstructive disease, although restrictive diseases are both less common and less receptive to medical management.
Obstructive ventilatory disease would include chronic obstructive pulmonary disease (COPD) which is important contributor to mortality and morbidity.
Pre-existing pulmonary dysfunction adds to the likelihood of postoperative respiratory complications which may appear during the initial phases post surgery.
Outcome may be enhanced by identifying reversible ventilation defects (RVD) in the preanesthetic phase.
1Different respiratory defects present also is unique clinical characteristics and accordingly this condition allows for the development of management methods to enhance physiological function.
In order to develop the appropriate anesthetic plan, interpretation of respiratory (pulmonary function tests) status is a central consideration.
Pulmonary Function Tests: Spirometry
1Spirometry represents a set of tests which is useful in pulmonary function assessment. Spirometric analysis is probably the most commonly used technique to distinguish between restrictive and obstructive disease. Attainment of quality results may be challenging for patients with COPD since significant effort is required in the test itself.
1A basic element of the task is to determine time dependency of lung gas forced expiration parameters. This approach allows total lung capacity (TLC), residual volume (RV) and other parameters to be assessed. Spirometry allows computation of forced vital capacity (FVC), forced expiratory volume at one second (FEV1), FEV/FVC ratio, as well as the midflow rate which is defined as the forced expiratory flow (FEF) from 25% to 75% of the vital capacity; this FEF is represented as FEF25-75, and finally the forced expiratory flow at 50% of the vital capacity, represented as FEF50.
1A spirogram is based on the relationship between volume and time during forced exhalation. This process is repeated in order to ensure that a "best effort" has been obtained. Calculation of the parameters noted above are derived from this analysis. In order to assess the efficacy of bronchodilator medication in a particular patient, individual spirometric results would be repeated following bronchodilator administration.
|
|
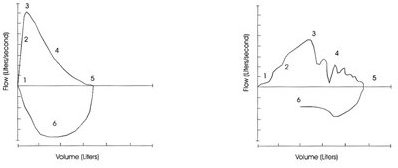
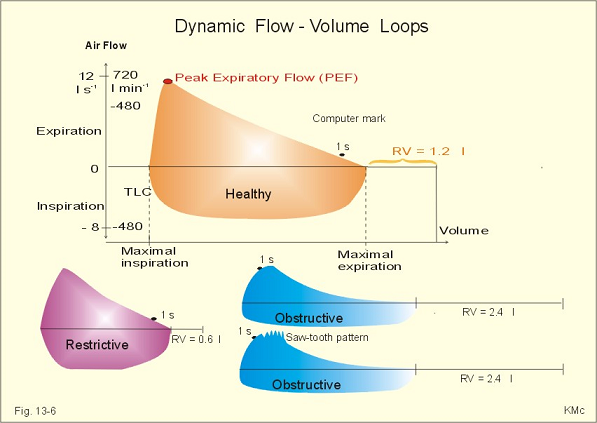
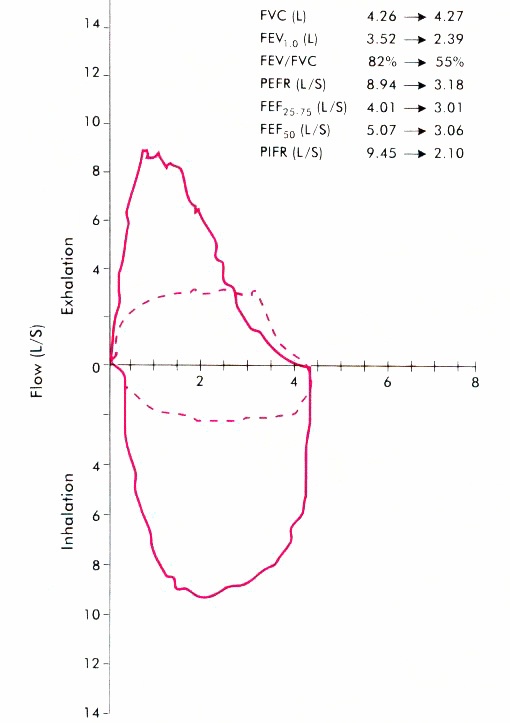
The above graph provides an alternative to the spirogram plot of volume vs. time, this time plotting change in flow vs.lung volumes--a relationship which results in a flow-volume loop graph. In this process there is a coupling of the inspiration step (RV back to TLC) which follows exhalation (TLC to RV).
Information essentially similar to that obtained from spirometry is available using this graphical transform allowing estimation of FVC, FEV1, peak expiratory flow rate (PEFR), FEF25-75, and FEF 50.
This transform may be particularly sensitive with respect to early chronic obstructive lung disease detection because reduced flow associated with low lung volumes is observable prior to FEV1 or FEV1/FVC ratio changes.
Note in the graph above, there is a slight concave shape associated with the last part of the exhalation curve. This concavity is consistent with an early airflow obstruction (small airways), although normal FEV1 & FVC values are noted.
Principal advantage of flow volume loops vs. typical standard spirometric descriptions is the ability to identify the probable obstructive flow anatomical location.
The flow volume loop provides the basis for a discriminating analysis since distal airway obstruction can be separated from obstructions occurring in the extrathoracic upper airway.
This discrimination is possible since both inhalation and exhalation is represented on the same graph (loop).
With respect to anesthesia, the extrathoracic obstruction (meaning upper airway, larynx, trachea) is especially important. An obstructing lesion located at these sites can limit airflow in a fixed way and would be identified during the inhalation component on the flow-volume loop. Stridor (inspiratory) is the result.
|
|
2http://asthma.about.com/library/weekly/aa090897.htm
The above flow volume loop is consistent with airway obstruction, as indicated by the concave shape of the upper right portion of the graph. The red line would be the predictive value taking into account parameters such as patient height, weight, age, and ethnicity. Noteworthy points along the graph have been numbered and are defined as follows.
1. Peak expiratory flow rate (PEFR). The value of PEFR is that it allows assessment of expiratory muscle strength, large airway patency (trachea, main bronchi) as well as overall test validity. An asthmatic patient may have normal or decreased PEFR values.
2. Forced Expiratory Flow at 25% (FEF25%) occurs when 25% of the total volume (FVC) has been exhaled. If maximal patient effort in exhalation is being maintained, then this flow rate would be reflected of flow through medium-size to large bronchi. This value in concert with the FEF 75% gives the range FEF25%-75%, which overall represents the middle half of FVC. This range appears less dependent on patient effort and is perhaps more reflective of the presence or absence of small airway obstruction. The FEF25%-75%is sensitive to the total volume exhaled (FVC) and appears to exhibit significant variability.
Generally, patients with asthma may have decreased FEF25% with the extent of the decreased dependent on the magnitude of the inflammatory response and extent of bronchoconstriction.
The effect on FEF25% may be noticeable and variable expiratory flow rates in may be observed in the absence of overt patient symptoms.
3. FEF50% is being expiratory flow rate at the 50%.relative to the total volume (FVC) which will be exhaled.
FEF50% may be indicative of medium-small airway caliber and may be used as an alternative to FEF25%-75%.
4. FEF75% is the flow rate at the 75% relative to the total volume to be exhaled (FVC).
This point reflects small airway status and is used in the FEF25%-75% calculation.
Decreased values in FEF75% would be expected in the asthmatic patient, even if symptoms are not apparent.
This result is expected because most chronic pulmonary diseases are manifest initially in the smallest airways, which contribute significantly towards the end of the expiratory part of the flow volume loop.
5. Forced Inspiratory Flow at 25% of FVC (FIF25%). This point is defined as the flow rate at the 25 percent point relative to the total volume which will be inhaled. This flow rate will not be particularly important in understanding for assessing the asthmatic state. However, it is an important value for anesthesiology because it indicates upper airway obstruction. Reduced inspiratory flow rates may be due to obstructions in the mouth, upper & lower pharynx, larynx, and vocal cords.
6. Peak Inspiratory Flow Rate (PIFR) is defined by the fastest flow rate noted during the inspiratory cycle.
7. Forced Inspiratory Flow at 50% of FVC (FIF50%) represents the flow rate at the 50% point relative to the total volume to be inhaled.
8. Forced Inspiratory Flow at 75% of FVC (FIF 75%) represents the flow rate at the 75% point relative to the total volume to be inhaled.
9. Forced Expiratory Volume at the 0.5 seconds (FEV 0.5). This value defines the amount of air exhaled (assuming maximal effort) in 0.5 seconds.
10. Forced Expiratory Volume after 1 seconds (FEV1). At maximal effort, FEV 1 defines the air volume exhaled within the first second. Following administration of bronchodilator agent, FEV 1 values tend to improve in the asthmatic patient.
|
|||||
|
|
|
|
The purpose of the tests is to allow discrimination principally between obstructive and restrictive disease, recognizing that both elements may be present in a given patient although one aspect may well be dominant.
Restrictive ventilatory dysfunction (RVD) would be suggested by a reduction of forced vital capacity (FVC) while retaining normal values of FEV1 and FEV1/FVC. This pattern would be consistent with extrinsic RVD, such as caused by obesity, kyphoscoliosis, and paralyzed diaphragm. This pattern is also consistent with intrinsic RVD caused by for example interstitial fibrosis.
Obstructive ventilatory dysfunction (OVD) with the manifest with retention of normal FVC (initially) with decreasing FEV1 and FEV1/FVC ratios appearing early. Eventually, FVC values will decline late in the disease.
An important aspect in spirometric and flow volume loop analysis is the issue of reversibility.
In terms of preoperative assessment, the ability to improve pulmonary function by the use of, for example, bronchodilator treatment is an important consideration. In patients with OVD, proven bronchodilator-mediated improvements midflow flow rates [FEF25-75; FEF50] would be important to know preoperatively since bronchodilators might be used as part of the anesthetic plans. Bronchodilator-mediated improvement might be expected in patients with asthma or chronic bronchitis.
More broadly, management of extra- or intrathoracic airway obstruction by surgical intervention may be more efficacious in the context of flow volume loop information.
|
1Upper airway obstruction: Flow-volume loop signature
1Solid line above would be the normal flow-volume loop which may be contrasted to the "box-shaped loop" which is consistant with a fixed upper airway obstruction.
Note reduction in peak flow midflow values
1Restrictive Ventilatory Defects (RVD)
Restriction of alveolar ventilation a mechanical forces defines RVD. The forces that resist both inspiration and expiration are present in restrictive disease. The categories of RVD are (a) intrinsic (b) extrinsic. The category diseases that represent RVD include: pleural and chest wall disorders (constricted), neural disorders and primary alveolar and supporting tissue disease.
Clinical presenting characteristics:
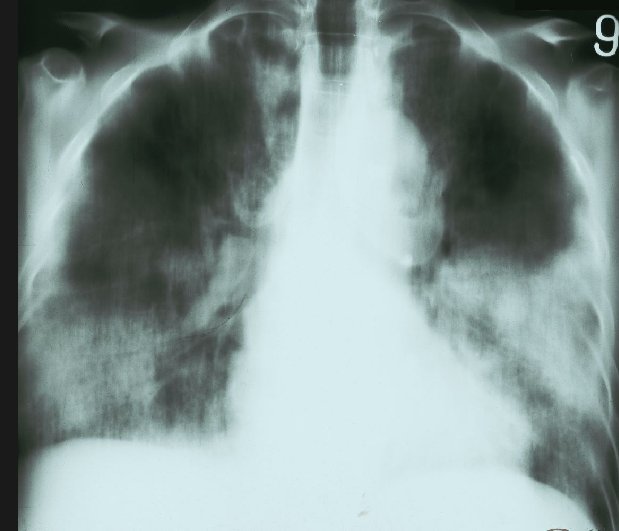
Tachypnea and dyspnea are particularly present in the postoperative patient with pain and with RVD. Chest radiographic imaging indicates interstitial patterns with reduced lung volumes. Arterial hypoxemia even in rest may be present in severe disease and arterial hypoxemia can be worsened by exercise. Altered pulmonary arterial pressure may be induced by chronic hypoxemia and increased pulmonary arterial pressure itself adds risk to other cardiovascular risk factors, overall resulting in increased susceptibility to right-sided heart failure.
In RVD, pulmonary function tests indicate parallel and proportional decreases in both FVC and FEV 1 [this result is different from that obtained in OVD in which obstructive disorders are present even with normal ventilatory mechanics and as a result of pulmonary function tests note that FEV 1 reduction does not parallel reduced FVC.
|
|
4Pulmonary test characteristics:
Low total lung capacity
A low functional residual capacity
A low residual volume.
The forced vital capacity (FVC) may be low; however, FEV1/FVC is often normal or greater than normal due to the increased elastic recoil pressure of the lung.
Since lung inflation requires large pleural pressure drops, deep breaths are difficult for patients with RVD; These patients exhibit shallow and rapid breathing patterns.
As noted earlier, RVD and OVD may exist concurrently with mixed spirometric patterns. Reversible components of mixed pathologies may involve administration of antibiotics or steroid or bronchodilator drugs.
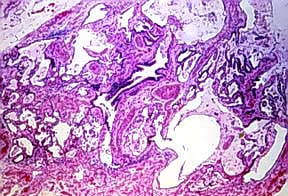
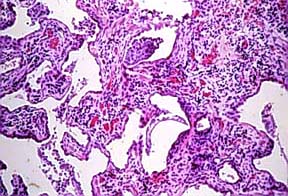
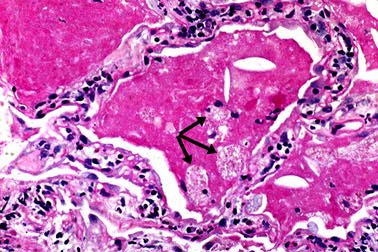
Pathological characteristics of intrinsic RVD are reflected in alveolar membrane thickening which then impedes gas diffusion. This effect would be seen in pulmonary fibrosis, pulmonary alveolar proteinosis, bronchiolitis obliterans and pneumonia.
|
1Extrinsic RVD occurs when alveolar volume is reduced due to compression by mass effect (such as tumor, blood, effusion) or if there is a reduction in thoracic compliance which causes a reduced number of ventilated alveoli.
Examples of such causes include scoliosis, neuromuscular diseases, obesity, and scoliosis.
Obstructive manifestation of sarcoidosis presents later in the disease process.
A restrictive ventilatory disease which is sometimes reversible is adult respiratory distress syndrome (ARDS), which is associated with a 50% mortality rate. ARDS may frequently present in the perioperative time-frame in the patient subgroup that exhibits a history of sepsis, severe trauma, pancreatitis, or multiple organ system failure.
1The importance of restrictive ventilatory defects is reflected in two elements -- (1) the diagnostic and management challenge and (2) their importance as representative of reversible restrictive alterations following anesthesia and surgery, particularly intrathoracic and upper abdominal surgery.
RVD may be induced by pain, residual neuromuscular blockade, abdominal wound dressings, thoracic wound dressings, and diaphragmatic as well as chest wall neuromuscular dysfunction.
These factors may be individually addressed preoperatively were perioperatively to reduce the likelihood of RVD-induced postoperative complications. For RVD and OVD, the process of anesthesia and surgery may induce mechanical ventilatory restrictions that are inflected on pre-existing, usually restrictive, ventilation abnormalities.
1Obstructive Ventilatory Defects (OVD)
Obstructive ventilatory defects (OVD) represent pathologies which increase airflow resistance due to obstruction, during the respiratory cycle.
This condition may be acute or chronic but in either case obstruction may be intralumenal, extralumineal or both. These obstructive defects tend to be more likely reversible then those found in restrictive ventilatory disorders.
Accordingly, OVD can be discussed in terms of specific medical intervention.
Examples of OVD causes include obstructing airway tumors, anatomical pathologies such as vocal cord paralysis or tracheobroncheomalacia as well as well-known and obstructive pulmonary diseases such as chronic bronchitis, asthma, and emphysema.
COPD is used as a descriptor providing the most generalized and common framework for classifying these disorders.
All OVD in presentations exhibits airflow resistance during exhalation secondary to decreased airway caliber.
The reduction in airway diameter may be due to glottic or subglottic mass obstruction, accumulation of mucus secretion, local inflammation, smooth muscle hypertrophy and bronchiolar and alveolar structural weakness.
The COPD patient, distinct from the patient with upper airway or pharyngeal-level obstruction, does not exhibit difficulty during inspiration since inspiratory resistive components cannot contribute significant additional respiratory work.
However the resistive forces associated with expiration become important because of air trapping behind obstructive small caliber airways.
11In terms of measures of respiratory function, OVD manifests as a reduction in forced expiration (low FEV1/FVC).
Patients experiencing active asthma or emphysema will exhibit both high residual volume and functional residual capacity and low vital capacity.
By contrast, patients with bronchitis will probably exhibit more normal lung volumes.
|
|
|
|
|
|
|
|
|
|
|
|
1Kopp, VJ and Boysen, PG "Evaluation of the Patient with Pulmonary Disease" Chapter 13, in Principles and Practice of Anesthesiology, 2nd Edition, Longnecker, D.E., Tinker, J.H, and Morgan Jr, G.E., eds), pp 232- 242, Mosby, St. Louis,1998.
3University of Western Ontario, Department of Pathology; maintained by C.J. Gibson-
4Johns Hopkins Interactive Restrictive Physiology, "Restrictive Ventilatory Defect" Copyright © 1995 Johns Hopkins University
5Pulmonary Alveolar Proteinosis (Ch. 79); Pulmonary Disorders (Section 6); The Merck Manual of Diagnosis and Therapy,
6Michael P. D'Alessandro, M.P and Yasayuki Kurihara,Y.,n Chest X-Ray: Pulmonary Alveolar Proteinosis, University of Iowa
7Department of Pathology, UCSF,
8Johns Hopkins Interactive Restrictive Physiology, "Emphysema" , Copyright © 1995 Johns Hopkins University
9Johns Hopkins Interactive Restrictive Physiology, "Bronchitis"Copyright © 1995 Johns Hopkins University
10Johns Hopkins Interactive Restrictive Physiology, "Asthma" Copyright © 1995 Johns Hopkins University
11Johns Hopkins Interactive Restrictive Physiology, "Obstructive Ventilatory Defects" Copyright © 1995 Johns Hopkins University
12 Dweik, R.A. and McCarthy, K., "Pulmonary Function Testing" emedicine,
13 "Tracheomalacia": Medline Plus Health Information (Encyclopedia)
14 Polsdorfer, J. Ricker, Relapsing Polychondritis. Health Topics A-Z; secondary sourcesGilliland, Bruce C. "Relapsing Polychondritis and Other Arthritides." Harrison's Principles of Internal Medicine, edited by Antony S. Fauci, et al. New York: McGraw-Hill, 1998.: Schumacher, H. Ralph. "Relapsing Polychondritis." Cecil Textbook of Medicine, edited by J. Claude Bennett and Fred Plum. Philadelphia: W. B. Saunders, 1996.
15Tso, A.S, Chung, HS, Wu, C-Y, Li, J-Y, Hong, C-L, Yang, M-W, Lui, P-W., Anesthetic Management of a Patient with Relapsing Polychondritis-A Case Report. Acta Anaesthesiol Sin 39: 189-194, 2001.
16Waheed, N K, Relapsing Polychondritis
17Wyser, C, Stulz, P, Soler, M: Prospective evaluation of an algorithm for the functional assessment of lung resection candidates. Am J. Respir Crit Care Med 1999; 159-5 Pt 1_: 1450-6, (second sourced from reference 12 above)
18Warnock M.L. and McCowin, M.J. "Emphysema" (Overview of Pulmonary Pathology) in Practical Pathology of Chest Disease--Case Studies
19Introduction to Clinical Radiology, Radiology Pathology - BMS 5191, University of Florida College of Medicine
20Michael P. D'Alessandro, M.P and Yasayuki Kurihara,Y., Emphysema (Classic) on CXR, University of Iowa
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |
.jpg)
.jpg)