Anesthesia Pharmacology Chapter 14: General Anesthesia
![]()
![]()
|
|
|
|
|
|
Depth of anesthesia depends on the agent's partial pressure (tension) in the brain.
The drug's partial pressure is indicative of the drug's concentration at the target site (the brain).
Anesthetic physico-chemical properties as well as hemodynamic and pulmonary function are important determinants of both time to onset of the drug and recovery from the drug.
Four factors determine the partial pressure in arterial blood and therefore in the brain:
Anesthetic concentration in the inspired air
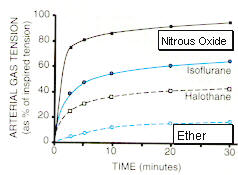
The rate of increase in tension (concentration) of anesthetic in arterial blood is determined in part by the concentration of the agent in the inspired gas.
This rate of increase in arterial gas tension is not the same anesthetic to anesthetic.
Differences between agents have to do with differing physico-chemical properties which are manifest as differences in solubility.
The anesthetic molecule interacts with water molecules in the blood and depending on the anesthetic molecular structure, the drug will be relatively more or less soluble.
Lower anesthetic solubility in blood results in the "blood" compartment becoming saturated with the drug following fewer gas molecules transferred from the lungs into the blood.
Once the "blood" compartment is saturated with anesthetic, additional anesthetic molecules are readily transferred to other compartments, the most important one of which is the brain.
|
|
Pulmonary ventilation
The rate of increase in tension (concentration) of anesthetic in arterial blood is determined in part by respiratory minute volume.
The higher the minute volume the more gas per unit time is delivered to the alveoli for transfer to arterial blood.
Accordingly, overventilation during induction can increase the rate of rise of arterial blood anesthetic gas tension.
By contrast, respiratory depression can delay the attainment of brain anesthetic concentrations.
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodmanand Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p. 298.
Transfer of the gas from the alveoli to the blood: In the absence of ventilation-perfusion mismatching* three factors determine how quickly anesthetics pass from the inspired gas to the blood:
Anesthetic solubility in the blood
Inhalational agent solubility in blood is the single most important factor in determining the speed of induction and recovery
The more soluble an agent is in the blood the more must be dissolved to raise its partial pressure (tension).
For a very soluble agent, the partial pressure rises slowly.
An example of a very soluble agent is methoxyflurane (blood:gas partition coefficient = 12). Induction times may be prolonged.
An example of a sparingly-soluble agent is nitrous oxide (blood gas partition coefficient = 0.47). The arterial blood partial pressure for nitrous oxide will rise rapidly
*Ventilation-perfusion mismatching refers to the condition in which regions of the lung may not be functional and as a result blood flow is shunted away from these regions. The extent to which blood is not shunted as in effect on the rate of rise of arterial anesthetic tension because blood flowing through non-functional lung regions cannot pickup anesthetic molecules.
Pulmonary Blood Flow
Pulmonary blood flow is closely related to cardiac output.
Higher pulmonary flow results in an initial relative decrease in the rate of rise of anesthetic tension (since there is less time for transport of gas from the alveoli into blood). Despite this effect, there is little influence of pulmonary flow on the total time to reach equilibrium
Partial Pressures in Arterial and Mixed Venous Blood
The amount of dissolved anesthetic in mixed venous blood returning to the lung influences the rate of transfer of anesthetic gas into blood.
Initially, when the process is far from equilibration (little dissolved gas), transfer rates are highest. We can appreciate this relationship since the flux of molecules across the membrane will be influenced by the concentration gradient (C1 - C2). As the difference between becomes less the flux will be reduced. Recalling Fick's equation--
Flux (molecules per unit time) = (C1 - C2) · (Area ·Permeability coefficient) / Thickness
Therefore, as equilibrium is approached and the concentration difference is reduced, the net flux (in the direction of increasing arterial gas tension) is reduced.
With time, equilibrium is approaches and net transfer rates decline, accounting for the relatively slower rise in final portions of arterial tension curves.
|
|
(Adapted from :Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodmanand Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) The McGraw-Hill Companies, Inc.,1996, pp.297, Figure 13-1.)
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodmanand Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p. 298.
Ezekiel, M.R., Handbook of Anesthesiology, Pharmacology, Current Clinical Strategies Publishing, 1997, p. 26.
Transfer of the gas from the blood to body tissues (brain)
Solubility of the gas in tissues is an important factor.
For a relatively lipophilic drug and given the brain's high lipid content, solubility properties favor transfer
Rate of delivery of anesthetic to tissue is clearly an important aspect since transfer cannot occur unless the drug is in fact delivered to the target tissue.
Difference in partial pressures (concentration) between arterial blood and tissue represent the concentration gradient C1 - C2 which influences the rate of transfer.
General anesthetics are dangerous with therapeutic indicies of about 2 - 4, i.e. a dosage only two to four times above that required to produce anesthesia can produce circulatory failure.
Although the brain is the site of action, anesthetic potency is measured on the basis of an alveolar gas concentration that produce immobility in 50% of patients exposed to painful stimuli. Classically, the painful stimulus is defined as associated with an abdominal incision.
Therefore, the minimum alveolar concentration (MAC) is the alveolar anesthetic concentration at one atmosphere (760 mm Hg) preventing movement in 50% of patients exposed to noxious stimuli.
The 95% confidence ranges for MAC correspond to about the MAC value +/- 25%, which provides a rationale for the clinical dose of about 1.2-1.3 MAC which would be expected to prevent overt patient reaction during surgical stimulation.
A central question is whether or not the patient during anesthesia might be aware of the procedure or might recall it. Probably such awareness or recall is highly unlikely if the anesthetic is administered in the 1.2-1.3 MAC range.
MAC values associated with loss of recall or self-awareness would be about 0.4-0.5 MAC.
An example would be the use of nitrous oxide in the context of a dental procedure.
In this case patients receiving 50% nitrous oxide, which corresponds to about 0.45 MAC, do not recall the procedure.
EEG changes appear to correlate with loss of self-awareness.
This change corresponds to a shift in EEG dominance to the anterior electrode leads. At least in primates, the shift appears to occur at about 0.5 MAC and his associated with loss of consciousness
Waking up: The MAC value range at which a patient will open eyes upon command is about 0.15-0.5 MAC.
Suppression of autonomic adrenergic responses to painful stimulation:
At certain times during the surgical procedure it is likely that an increase in painful stimulation will occur -- most apparently at the time of initial incision but also during subsequent manipulations.
MAC values which are sufficient to ensure patient non-overt responsiveness to pain are not sufficient to prevent adrenergic responses to pain. These responses are manifested as increasing blood pressure and heart rate.
To suppress these responses requires an increase in MAC by about 50%. Therefore, an anesthesia provider, anticipating a noxious stimulation, such as the initial incision, can largely prevent or certainly reduce the hemodynamic response by increasing temporarily the delivered anesthetic concentration.
Rules concerning the summation of MAC values when multiple agents are used:
If the end point is preventing patient movement in response to painful stimulation, MAC values of multiple, concurrently administer drugs are roughly additive. This means that 1 MAC may be obtained by combining, for example, 0.5 MAC nitrous oxide with 0.5 MAC of a potent inhalational agent.
If one considers endpoints other than blocking patient movement response to painful stimulation, the summation rule described above may not apply.
For example, if the end point were a hypotensive response, then 0.6 MAC nitrous oxide + 0.6 MAC halothane (Fluothane) produces less hypotension than 1.2 MAC halothane (Fluothane) alone.
The reason for this is that halothane (Fluothane) is a more potent vasodilator and causes greater myocardial depression than nitrous oxide.
In this case the basic pharmacological differences between the drugs in relation to the organ system physiology must be taken into consideration.
If blockade of patient movement response to painful stimulation is the primary MAC definition, then other MAC response relationships can be considered secondary. Examples of secondary MAC responses include:
MAC-arrhythmias
MAC-hypotension (noted in the example above)
MAC-tachycardia
These secondary responses or effects would not be expected to obey the "additive" rule which appears to apply to the primary end point of patient movement response to noxious stimulation.
MAC values: age dependencies
Anesthetic MAC values change with the age of the patient.
The general rule is that, with aging, MAC values decrease and that the rate of change (rate of decrease) does not appear dependent on which agent is considered.
The rule of thumb is that the MAC value decreases by about 6% per 10 years (22% decline in MAC from age 40 to age 80; 27% decline in MAC from age 1 to 40)
MAC values typically used refer to 40 year-old individual
halothane (Fluothane): 0.75%
isoflurane (Forane): 1.17%
enflurane (Ethrane): 1.63%
sevoflurane (Sevorane, Ultane): 1.8%
desflurane (Suprane): 6.6%
nitrous oxide: 104%
An equation which allows estimation of the change in MAC as a function of difference in age in years from 40: MAC =a(10bx) where a is the MAC value at age 40 for the particular anesthetic, x is the difference in cage of the patient from 40 and b = -0.00269.
Rationale for using alveolar concentrations rather than brain levels
Alveolar concentrations are easy to measure accurately.
At equilibrium the partial pressure of the gas in the lung is about the same as in the brain.
Blood and brain anesthetic concentrations rapidly equilibrate.
More about MAC
MAC values are not dependent on the nature of the noxious (painful) stimulus.
MAC values are relatively insensitive to sex, height, weight, and duration of anesthesia, although age and temperature do affect MAC.
On the other hand, there are factors that increase the apparent MAC value for an anesthetic. These factors include:
hypernatremia
hyperthermia
chronic ethanol abuse
Increased central neurotransmitter level which might be associated with monoamine oxidase inhibition, L-DOPA administration (presumably given to manage Parkinsonism), acute d- amphetamine administration,ephedrine administration or cocaine use.
Not surprisingly there are many factors which decrease the apparent MAC value for an anesthetic. These factors include:
|
|
|
*A decrease in central neurotransmitter level can be caused by many drugs, including chronic d- amphetamine use, reserpine (Serpasil), alpha-methyldopa)
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodmanand Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p. 298.)
(Ebert, Thomas J and Phillip G Schmid III, Inhalation Anesthesia in Clinical Anesthesia (4/e),edited by Paul G. Barash, Bruce F. Cullen and Robert K. Stoelting, Lippincott Williams and Wilkins, Philadelphia (c) 2001.)
![]()
Pharmacological and clinical differences among the inhalational anesthetics
|
|
|
|
Halothane: (Flurothane)
Overview:
Halothane causes unconsciousness; however, does not provide adequate analgesia.
Halothane (Fluothane) may not adequately suppress visceral reflexes or provide adequate muscle relaxation for surgery
Halothane (Fluothane) is associated with reversible reduction in glomerular filtration rates (GFR)
Halothane Advantages:
Halothane (Fluothane) is relatively potent and is nonflammable.
This drug's low blood:gas partition coefficient explains both relatively rapid anesthesia induction and recovery from anesthesia
Halothane (Fluothane) can be used to provide controlled hypotension to reduce/manage bleeding
Halothane Disadvantages
Halothane (Fluothane) is associated with unpredictable hepatitis occurrences
Significant myocardial depression is observed with halothane (Fluothane)
Halothane Status:
While halothane (Fluothane) is used in pediatric anesthesia, it is infrequently used in adults due to the availability of isoflurane (Forane), enflurane (Ethrane), sevoflurane (Sevorane, Ultane) and desflurane (Suprane). These agents exhibit relatively more favorable pharmacological properties.
|
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 313. |
Enflurane (Ethrane)
Overview
Enflurane anesthesia: provides unconsciousness
Slight stimulation of salivation and tracheobronchial secretions
Enflurane is typically avoided in epileptic patients because of a CNS excitatory property occasionally seen.
May provide adequate muscle relaxation greater than seen with halothane; perhaps adequate for abdominal procedures
Reversible reduction of GRF
Fluoride (a metabolite of enflurane) usually does not reach levels required for kidney toxicity
Enflurane Advantages
Rapid, smooth adjustment of depth of anesthesia with limited effects on pulse or respiration.
Compared to halothane: less arrhythmias, nausea, post-operative shivering and vomiting
Relaxation of skeletal muscles may be adequate for surgery
Enflurane Disadvantages:
possible concern about its use in patients with seizure disorders
Enflurane Status: Enflurane is used as an inhalational agent for adults; but is not widely used for pediatric cases.
|
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 311 - 315. |
Isoflurane (Forane)
Overview:
Isoflurane anesthesia: provides unconsciousness
By contrast to enflurane or halothane, cardiac output is well maintained with isoflurane.
Initially, until deeper levels of anesthesia are reached, isoflurane stimulates airway reflexes with attendant increases in secretions, coughing and laryngospasm. (greater with isofluorane than enflurane or halothane)
May provide adequate muscle relaxation greater than seen with halothane which may be adequate for abdominal procedures.
As with enflurane, isoflurane relaxation of uterine muscle is not desirable if uterine contraction is required to limit blood loss.
Reversible reduction of GRF;
Unlike enflurane, convulsive activity has not been seen with isoflurane.
Isoflurane Advantages:
Rapid, smooth adjustment of depth of anesthesia with limited effects on pulse or respiration.
Depth of anesthesia is easily controlled.
No hepatic and renal toxicity
Cerebral blood flow and intracranial pressure are readily controlled.
Relaxation of skeletal muscles may be adequate for surgery
Arrhythmias are uncommon.
Isoflurane Disadvantages:
As with halothane and enflurane, isoflurane may cause malignant hyperthermia
Isoflurane Status:
Isoflurane may be the most widely used inhalational agent.
|
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 315 - 317. |
Desflurane: (Suprane)
Overview:
Desflurane anesthesia: provides unconsciousness
Very limited solubility (similar to nitrous oxide) allows rapid onset and recovery and precise controlled anesthesia.
Since laryngospasm and coughing are associated with desflurane administration, this agent is typically administered following induction by an i.v. drug.
Recovery twice as rapid as for isoflurane.
May not provide adequate muscle relaxation
Circulatory effects are similar to isoflurane: cardiac output is preserved.
Reversible reduction of GRF
Seizure-like activity is not observed.
Malignant hyperthermia may occur with desflurane.
No renal toxicity
Some muscle relaxation is present, allowing intubation, and lessening dosage requirements for muscle relaxants.
|
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E,Molinoff, PUB., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 317 -318. |
Sevoflurane (Sevorane, Ultane)
Overview:
Low blood solubility; high potency allow excellent anesthesia control.
Pharmacological properties resemble desflurane
Very commonly used.
Increase fluoride levels rarely associated with kidney or renal damage.
Compared to desflurane, sevoflurane is more extensively metabolized, releasing more fluoride.
|
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 318 - 319. |
Overview:
With a MAC value of 105%, nitrous oxide, by itself is not suitable or safe as a sole anesthetic agent.
Nitrous oxide is an effective analgesic.
Effective: Nitrous oxide in combination with:
Thiopental for induction
A skeletal muscle relaxant
and hyperventilation to reduce CO2
Despite the relative insolubility of nitrous oxide, large quantities of gas are rapidly absorbed due to its high inhaled concentration. This concentration effect speeds induction as fresh gas is literally drawn into the lung from the breathing circuit.
Since nitrous oxide is often administered with a second gas, the second gas effect also enhances the rate of induction.
If administration of nitrous oxide is abruptly discontinued, rapid transfer of NO from blood and tissues to the alveoli decreases arterial tension of oxygen. This process is diffusional hypoxia.
Nitrous oxide should NOT be used if pockets of trapped air are suspected in the patient (e.g. following a pneuomoencephalogram) or in an occluded middle ear, because of exchange of NO with nitrogen with attendant gas expansion.
Nitrous oxide has minimal effects on the circulation compared to the other inhalational agents with which it is co-administered.
Nitrous oxide by itself has minimal effects on respiratory drive.
Minimal skeletal muscle relaxation.
No significant effects on the liver, kidney, or GI tract.
Nitrous Oxide Advantages:
Excellent analgesia
Nonflammable
Very rapid onset and recovery
Little or no toxicity
Use as an adjunct to other inhalational agents allows reduction in their dosage
Nitrous Oxide Disadvantages:
No skeletal muscle relaxation
Weak anesthetic
Air pockets in closed spaces expand
Post-anesthesia hypoxia (diffusion hypoxia)
Not suitable as a sole anesthetic agent
Concentration and Second Gas Effect
Concentration Effect
If the concentration of an anesthetic gas is high, the rate of increase of gas tension in arterial blood is high.
For example, if 75% nitrous oxide and 25% oxygen were administered, the rate of uptake of gas may be 1 liter/min.
As this volume of gas is removed from the lung, fresh gas is pulled into the lung from the breathing circuit of the anesthetic delivery equipment.
This effect further increases the delivery of gas mixture and therefore the rate of rise of arterial tension for nitrous oxide is increased.
Speed of induction is therefore increased since the faster the arterial tension rises, the faster the rate of rise of gas tension in the brain.
This effect is dependent on the high concentration of inhaled gas.
Second Gas Effect:
If the above condition is present, but a second anesthetic gas is present, the rate of rise of arterial tension of the second gas is enhanced also.
If the first gas is nitrous oxide and the second enflurane, the concentration effect due to NO which pull more gas from the breathing circuit into the lung, pulls both fresh NO and fresh enflurane.
Thus the rate of rise of arterial tension of enflurane is faster as well.
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 300.
Reverse of the concentration effect: high rate of transfer of anesthetic from the blood and tissues to the alveoli.
This additional gas dilutes alveolar oxygen and can result in postoperative hypoxia.
This process is referred to as "diffusion hypoxia"
Lessened by administration of supplemental oxygen.
(Kennedy, S.K. and Longnecker, D.E., History and Principles of Anesthesiology In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, p 300.
![]()
![]()
|
|
|