|
|
|
Autonomic Pharmacology--Adrenergic Drugs
|
|
|
|
|
|
|
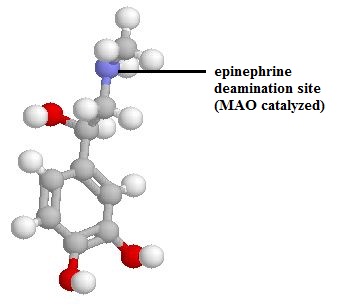
Epinephrine
Epinephrine undergoes rapid oxidation and conjugation in the liver following oral administration.
Therefore, for clinical effectiveness, other routes of administration must be utilized.
α-adrenergic receptor agonist properties of epinephrine cause localized vasoconstriction, which limits subcutaneous epinephrine absorption. Improved absorption can be obtained by intramuscular administration.
Both subcutaneous and intramuscular epinephrine injection are utilized for treatment of anaphylaxis.71
The subcutaneous route is often favored for "mild" reactions.
In the initial treatment of anaphylaxis, research findings suggest intramuscular epinephrine injection into the thigh is preferable compared to upper arm intramuscular or subcutaneous routes of administration. This conclusion was reached because peak plasma epinephrine concentration was higher following thigh administration (see figure below).71
|
|
|
Epinephrine undergoes rapid metabolism which results in its inactivation.
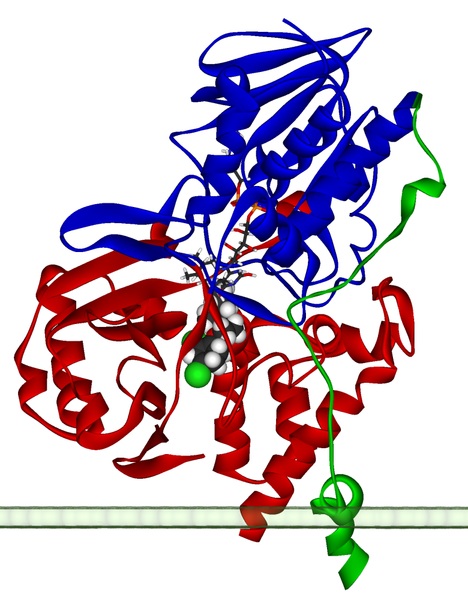
The hepatic enzymes monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT) are particularly important in epinephrine inactivation.
Monoamine oxidase catalyzes monoamine oxidative deamination. In a reaction that consumes oxygen, an amine group is removed forming the corresponding aldehyde and ammonia.
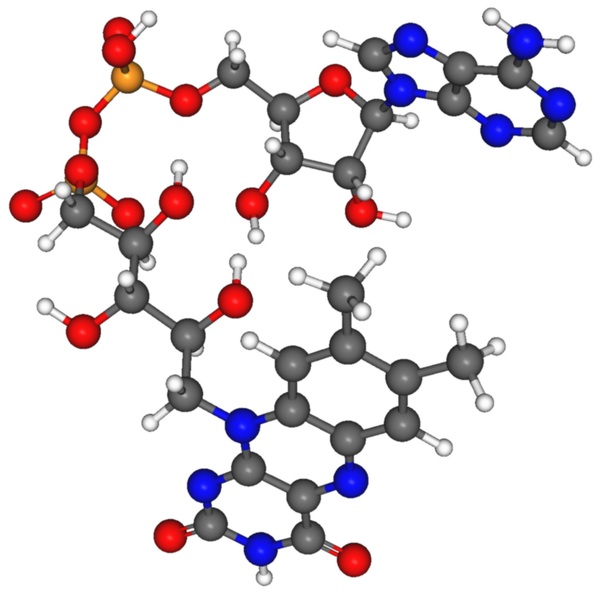
Monoamine oxidase enzymes contain a covalently linked cofactor FAD (flavin adenine dinucleotide) and therefore described as flavoproteins. The form of the reaction is shown below:72
 |
|
|
 |
|
|
 |
Inactivation of epinephrine and catecholamine neurotransmitters such as dopamine and norepinephrine also involves catechol-O-methyltransferase (COMT), an enzyme discoverd by Julius Axelrod in 1957.73
Methyltransferase enzymes catalyze methyl (CH3)-group transfers with the methyl group in this case provided by S-adenosyl-methionine (SAM).
|
|
|
COMT inhibitors such as tocapone (Tasmar, administered in combination with levodopa and carbidopa (Sinemet) and entacapone (Comtan, administered in combination with levodopa and carbidopa ) are used in management of Parkinson's disease. Entacapone does not exhibit anti-Parkinson's effects on its own.
In August 2010 the FDA notified healthcare professionals that evaluation of clinical trial data indicating patients taking a combination of carbidopa/levodopa and entacapone (the combination drug was Stalevo) might be an increased risk for cardiovascular events including heart attack, stroke, and cardiovascular death, compared to patients taking the combination product Sinemet (carbidopa + levodopa), was undertaken. It is suggested that the reader follow-up on the current status of this FDA evaluation.74
 |
 |
Various epinephrine formulations are available to accommodate differing routes of administration and/or clinical indications.
Epinephrine administration may involve:
subcutaneous injection
intramuscular injection
intravenous infusion
topical application
inhalation.
The intravenous route provides immediate effect and is administered cautiously with adequate dilution and slow injection.
Epinephrine suspensions are available to slow subcutaneous absorption and this preparation should not be injected intravenously.
Furthermore, the 1% (10 mg/ml; 1:100) formulation for use by inhalation must not be confused with the 1:1000 solution appropriate for parenteral use.
![]() Possible fatal consequences can ensue if 1:100 epinephrine solution
is administered parenterally.
Possible fatal consequences can ensue if 1:100 epinephrine solution
is administered parenterally.
Epinephrine is well known to be unstable and alkaline solution if exposed to air or light. Oxidation of epinephrine is indicated by a pink color (adrenochrome); subsequent polymer formation results in a brown appearance.
One contemporary major clinical use for epinephrine is in prompt management of hypersensitivity reactions to drugs and other allergens. Indications include treatment of anaphylaxis.4
Cardiac uses include helping to restore normal cardiac rhythm in patients in cardiac arrest..4
Epinephrine is the drug of choice for treating patients in cardiac arrest.4,58
Vasopressin may be considered if arrest continues following the first dose of epinephrine and vasopressin is considered a possible option to epinephrine.
 |
 |
In patients presenting with persistent ventricular fibrillation, amiodarone is likely the antiarrhythmic agent of choice, although its administration should be preceded by at least one epinephrine dose.
Epinephrine activates both α- and β-adrenergic receptors; however, the important epinephrine actions in this context appear mediated by α-receptor activation.
Mechanism of Action: The mechanism of action is based on epinephrine-mediated increases in systemic vascular resistance which secondarily improves both coronary and cerebral perfusion. Epinephrine administration along with β-adrenergic receptor antagonists proved helpful in resuscitation; whereas, epinephrine coadministration with α-receptor blockers were not helpful.58
2005 Guidelines indicate: "It is appropriate to administer a 1-mg dose of epinephrine (IV/IO (intraosseous) every 3 to 5 min during adult cardiac arrest (Class IIb). Higher doses may be indicated to treat specific problems, such as β-blocker or calcium channel blocker overdose."58a
β-adrenergic effects associated with epinephrine may precipitate, with repeated doses, recurrent ventricular arrhythmias; as a result, intravenous β-adrenergic receptor antagonists might be ineffective antiarrhythmic intervention during resuscitation should several epinephrine doses be administered.
High-dose epinephrine is not recommended.
Concerning vasopressin: this nonadrenergic peripheral vasoconstrictor has been recommended for use during cardiac arrest, although in two randomized clinical trials no increase in Return of Spontaneous Circulation (ROSC) was noted, when vasopressin was compared to 1 mg epinephrine.58
The 2005 Guidelines in its Advance Cardiac Life Support (ACLS) pulseless arrest algorithm notes that single vasopressin does may be substituted for the first 1 of 2 epinephrine doses.58,58a
The International Consensus Conference stated that there was insufficient evidence either to refute or support vasopressin uses an alternative to or in combination with epinephrine in any cardiac arrest rhythm.58
Vasocontrictors added to local anesthetic solutions78
Purpose of adding epinephrine to a local anesthetic solution: Increased duration: addition of epinephrine (1:2000,000 or 5 ug/ml) to cause vasoconstriction
Reduced systemic absorption
Higher anesthetic concentration near nerve fibers
Prolongation of conduction blockade (about 50% longer)
Reduced systemic absorption (by about 33%)
Factors influencing the effectiveness of epinephrine on local anesthesia: Dependencies --
Which anesthetic is used:
Reduced effect of epinephrine on duration of conduction blockade and systemic absorption comparing mepivacaine (Carbocaine) and etidocaine (Duranest) [these are more lipophilic] with lidocaine (Xylocaine), which is less lipophilic
More lipophilic local anesthetics will tend on their own to associate strongly with tissues
Level of sensory blockade needed for spinal or epidural anesthesia
Duration of lower extremity sensory anesthesia extended by epinephrine or phenylephrine (Neo-Synephrine); this effect is not observed for abdominal region anesthesia
Conditions: epinephrine (0.2 mg) or phenylephrine (Neo-Synephrine) (2 mg) added to mepivacaine (Carbocaine) or lidocaine (Xylocaine) -- placed in subarachnoid spaces
Spinal anesthesia -- tetracaine (pontocaine): duration of action extended by vasoconstrictors
Condition 1: epinephrine plus tetracaine (pontocaine) (6 mg, low-dose)- result: increase in spinal anesthesia success rate
Condition 2: epinephrine plus tetracaine (pontocaine) (10 mg, higher dose)- result: no increase in spinal anesthesia success rate
Prolongation of local anesthetic action (no effect by epinephrine on time-to-onset): Mechanisms --
Decreased systemic absorption
Increased local anesthetic concentration in the vicinity of sensory nerves
Increased uptake of the local anesthetic
Advantages of reduced local anesthetic systemic absorption:
Local anesthetic absorption rate more likely to match metabolic rate resulting in less local anesthetic systemic toxicity
Toxicities associated with systemic epinephrine absorption:
Local anesthetic + epinephrine: increased cardiac irritability which may cause an increased risk of cardiac arrhythmias
Increased possibility of hypertensive response in susceptible patients
Other agents which may be added to local anesthetics that affect duration of action
Dextran (low-molecular-weight) when added to local anesthetic solutions result in increased peripheral nerve block anesthesia duration (probably due to a reduction in local anesthetic systemic absorption)
Powerful vasoconstrictive actions of epinephrine, mediated by α1-adrenergic receptor activation, is the basis for effectiveness as a topical hemostatic agent. Bleeding surfaces in the mouth or bleeding peptic ulcers (visualized endoscopically) may be managed by epinephrine.
|
|
Disease or Drug Issue |
Selection Consideration |
| Stroke history | limit vasoconstrictor |
|
Cardiovascular conditions; and/or patient taking nonselective beta antagonists, antihypertensive drugs. |
limit vasoconstrictor |
| Hypoglycemic agents, insulin | limit vasoconstrictor |
| Hyperthyroidism | limit vasoconstrictor |
| Monoamine oxidase inhibitors (MAO inhibitors) | limit vasoconstrictor |
| Anticonvulsants, e.g. phenytoin | limit vasoconstrictor |
![]()
|
|
|
|
|
|
|
|
| This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |