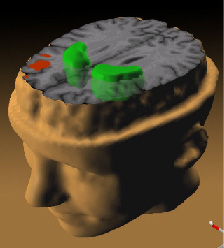
"While
patients performed a working memory task,
the less the prefrontal cortex (red)
activated, the more dopamine increased in
the striatum (green)."
|
|
|
Autonomic Pharmacology--Adrenergic Drugs
|
|
|
|
|
|
|
Dopaminergic Systems and Schizophrenia
Introduction:
Schizophrenia Overview:138
Schizophrenia is characterized by a number of different presentations including abnormalities in language, thinking, perception, social activity as well as affect and volition.
Clinical presentation often begins in late adolescence and symptoms of the condition develops slowly.
Initial characteristics might include social withdrawal and abnormalities in perception but evolve to include frequent delusions and hallucinations.
Symptoms have been categorized as either "positive" and "negative".
Positive symptoms include delusions or hallucinations and "conceptual disorganization"; whereas, negative symptoms include anhedonia (loss of ability to experience pleasurable emotions from typically pleasurable life experiences), reduced emotional expression, decreased social engagement, and concentration dysfunction.
Over time the positive psychotic symptoms tend to decline and individuals may regain a degree of social and occupational capacity.
Negative symptoms are dominant in about 33% of schizophrenic patients and tend to predict both poor long-term outcome and poor drug treatment responses.
Subtypes of schizophrenia include:
catatonic
paranoid
residual and
disorganized
Individuals may exhibit symptoms of more than a single type.
Catatonic-type patients present with notable changes in motor activity, negativism along with echolalia (repetition of sounds made by another individual) or echopraxia. (repetition of movements made by another).
Patients with paranoid-subtype tend to exhibit preoccupation with a specific delusional framework and do not qualify as having "disorganized-type" disease which is characterized by disorganized speech/behavior associated with superficial/silly affect.
An individual with "residual-type" schizophrenia would have been diagnosed with schizophrenia previously but is not presently exhibiting primary psychotic symptoms; however, there would be some remaining disorder symptoms.
Criteria for Schizophrenia
|
|
Epidemiology and Biology:138,136
Epidemiological assessments have considered a number factors that might predispose to schizophrenia development.
These considerations include adverse early developmental events, genetic predispositions, winter birth and increasing parental age.
Adverse early developmental events classify schizophrenia as a "neurodevelopmental" disorder, in which both structural and functional CNS effects might be expected.
With respect to genetics, genetic predispositions occur in some individuals who develop schizophrenia.
For example, schizophrenia is noted in about 6.5% of first-degree relatives of an affected individual.
Another example is that if both parents exhibit schizophrenia the likelihood for the child also to be afflicted is about 40%. For monozygotic twins the concordance rate is about 50%; moreover, this rate drops to about 10% for dizygotic twins.
Also, families that appear "schizophrenia-prone" exhibit higher risk for certain other psychiatric abnormalities which include schizoaffective disorder and schizotypal and schizoid personality disorders.
Schizotypal and schizoid personality disorder are used to describe individuals who exhibit a lifelong pattern of social and interpersonal abnormalities, especially difficulties in developing close interpersonal relationships, mild perceptual distortions, and eccentric behavior.
Genetics:138
Although major involvement of gene effects appear unlikely at present, some genes have been identified as associated with possible increased schizophrenia susceptibility.
These include:
neuregulin-1
dysbindin
proline dehydrogenase
D-amino-acid oxidase activator
Disruptive in Schizophrenia 1 (DISC1)
catechol-O-methyltransferase (COMT).
Some of these genes may be involved in glutaminergic (involving the neurotransmitter amino acid glutamate) function (neuregulin-1, dysbindin, and D-amino-acid acid oxidase. COMT, as described earlier, is involved in dopamine catabolism, whereas DISC1 is a scaffolding protein which may influence protein-protein interactions.
Pathophysiological Consideration: :138
Gestational and perinatal events appear associated with schizophrenia.138
These complications include prenatal nutritional inadequacy, fetal hypoxia, prenatal exposure to influenza during the second trimester and Rh factor incompatibility.
|
Neuroanatomical differences between affected and unaffected monozygotic twins (discordant for schizophrenia) suggest that manifestation of schizophrenia likely depends on two "insults" such as genetic susceptibility and environmental impact.138
The "environmental" effect might be regional hypoxia that might occur during brain development.
Neuroanatomical structures that have been identified as structurally or functionally abnormal include:
cortical atrophy combined with increased ventricular volume
decreased volume of several structures such as the amygdala, hippocampus, right prefrontal cortex, fusiform gyrus and thalamus
|
|
|
progressive decline in cortical volume, decreased thalamic and prefrontal cortical metabolism
abnormalities associated with the planum temporale
alteration in orientation, size, and cell density in both the hippocampus and prefrontal cortex along with a reduction in cortical interneurons.
These findings might be interpreted as associating schizophrenia with abnormalities in cortical striatal-thalamic circuitry which results in sensory filtering and attention abnormalities.138
Such abnormalities in sensory filtering and attention are associated with the schizophrenic profile in that afflicted individuals tend to be highly distractible, exhibit perceptual-motor speed deficits, show difficulty in the ability to shift attention and also have difficulty filtering out background stimuli to focus on a particular task.
Historically, chlorpromazine and reserpine were initial agents found helpful in management of schizophrenic, psychotic symptoms.136
Chlorpromazine was described as a "neuroleptic" drug, because it induces a cataleptic state in rodents and extrapyramidal syndromes (EPS) in humans.
Clozapine, discovered later, exhibited antipsychotic action but did not cause extrapyramidal symptoms (EPS).
The importance of this realization was that it was now viewed as possible to separate antipsychotic effects from the potentially serious extrapyramidal reactions.
Because of this discrimination, (the separation of antipsychotic action and absence of extrapyramidal symptom induction), clozapine was described as "atypical."
The major medical and socioeconomic consequence of the introduction of antipsychotic agents, including both typical and atypical variants, was an extraordinary change in disease management, now involving relatively brief hospitalizations instead of, sometimes, life-long confinement to a mental institution.
Neurological adverse effects associated with antipsychotic agents:136
Extrapyramidal symptoms (EPS) can be severe neurological side effects associated with administration of certain antipsychotic drugs.
Among EPS syndromes include:
Parkinson's syndrome
akathisia (restlessness)
acute dystonic reactions (spastic retrocollis and torticollis).
EPS-induced parkinsonism may be managed by anti-Parkinson's disease drugs (not L-DOPA) of the antimuscarinic type or sometimes with amantadine.136
This particular neurological effect appears self-limiting.
Akathisia and dystonic symptoms may also benefit by a similar pharmacological intervention, although alternatives include administration of sedating antihistamines with anticholinergic effects, as exemplified by diphenhydramine.
Tardive dyskinesia is a late-occurring neurological presentation characterized by abnormal choreoathetoid movements and is considered perhaps the most significant undesirable antipsychotic drug side effect.
Prior to the introduction of newer, "atypical"-type antipsychotic drugs the frequency of tardive dyskinesia presentations ranged between 20% and 40% in chronic treatment.
One of the most troubling aspects of this neurological side effect is that, if not treated early, the syndrome may be difficult to reverse.
Therapeutic management approach involves a discontinuation of the typical antipsychotic agent or occasionally risperidone or paliperidone with substitution of quetiapine or clozapine.
The latter two drugs are among those least likely to cause tardive dyskinesia.
Additional therapeutic management approaches may involve not only discontinuation or dosage reduction of the currently prescribed drug and substitution with one of the newer atypical agents but also, as a subsequent step, discontinuation of all agents with central anticholinergic effects, especially anti-Parkinson's agents and tricyclic antidepressants.
These two interventions may be adequate to improve the situation.
Should improvement not be forthcoming, an additional intervention may involve administration of relatively high dose diazepam (30-40 mg/day).136
Neurotransmitter-based models of schizophrenia:136
Serotonergic systems:136
Certain agent such as LSD and mescaline are well described hallucinogens.
Furthermore, these agents exert their hallucinogenic effects probably as a result of interaction with 5-HT (serotonin) receptors. Specifically, a serotonin receptor subtype, 5-HT2A, appears to be the receptor target.
The mechanism of action of the atypical antipsychotic drugs such as clozapine and quetiapine may involve their interaction with this receptor subtype.
Clozapine and quetiapine appear as inverse agonists at the 5-HT2A receptor in their binding decreases intrinsic, constitutive receptor activity.
These receptors appear participate in regulation of cortical, striatal, and limbic region dopamine release.
Glutamate systems:136
Another model of schizophrenia involves the neurotransmitter glutamate, which is the principal excitatory neurotransmitter in the brain.
Worsening of cognitive impairment and psychosis in schizophrenic individuals was observed following administration of ketamine and phencyclidine, both inhibitors of the NMDA receptor.
 |
 |
 |
 |
The NMDA receptor is a particular type of glutamate receptor with NMDA an abbreviation for N-methyl-D-aspartate. NMDA exhibits binding selectivity for the NMDA receptor compared to other glutamate receptors.
NMDA receptor activation is associated with increased ion channel conductance (increased ion flow).
Efficient ion channel activation requires both L-glutamate as well as a coagonist glycine. The glycine binding site is associated with the NMDAR1 (NR1) receptor subunit.143
|
|
|
"Stylised depiction of an activated NMDAR. Glutamate is in the glutamate binding site and glycine is in the glycine binding site. Allosteric sites that would cause inhibition of the receptor are not occupied. NMDARs require the binding of two molecules of glutamate or aspartate and two of glycine."143,145 |
The observation that ketamine and phencyclidine tended to worsen schizophrenic symptomatology led to the suggestion that diminished function of NMDA receptors associated with GABAergic interneurons result in reduced inhibitory influences on neuronal functions and therefore "contributed" to schizophrenia.136
Furthermore, reduced GABAergic activity could cause an inhibition of downstream glutaminergic neuronal activity which, in turn, could result in cortical neuron hyperstimulation via non-NMDA receptors.
Potential, future antipsychotic agents are in development with the idea that they may be effective through targeting of NMDA receptor systems, perhaps specifically the glycine, coagonist, binding site.136
Dopamine Systems: 136
Although perhaps no longer considered sufficient to explain schizophrenia in a complete way, the dopamine model for schizophrenia was the first neurotransmitter-based hypothesis.136
This model is still considered important in describing many aspects of the disease, including positive and negative symptoms and impairment of cognition.
The dopamine system is also important in helping to understand the likely mechanism of action of many antipsychotic medications.
Dopaminergic Pathways:
 |
| "Dopamine is transmitted via three major pathways. The first extends from the substantia nigra to the caudate nucleus-putamen (neostratum) and is concerned with sensory stimuli and movement. The second pathway projects from the ventral tegmentum to the mesolimbic forebrain and is thought to be associated with cognitive, reward and emotional behavior. The third pathway, known as the tubero-infundibular system, is concerned with neuronal control of the hypothalamic-pituitary endocrine system."82 |
Five important dopaminergic pathways have been identified in the brain.137
(1) the mesolimbic-mesocortical pathway is considered most closely related to behavior.148
For example, the system appears important in regulating behavioral responses to stimuli associated with feelings of reward and reinforcement.147
Projections in the system originate from neurons whose cell bodies are localized around the substantia nigra and and both in the limbic system and neocortex.
Anatomical structures constituting the mesolimbic pathway include:
(a) the ventral tegmental area (VTA), a part of the midbrain containing dopamine, GABA, and glutamate neurons.
(b) the nucleus accumbens localized in the ventral striatum and consisting of medium spiny neurons. The nucleus accumbens is divided into limbic and motor regions.
Medium spiny neurons receive input both from dopaminergic neurons of the ventral tegmental area and glutaminergic neurons localized in the hippocampus, amygdala, and medial frontal cortex.
The nucleus accumbens medium spiny neurons, when activated by these inputs, release GABA onto the ventral pallidum. The mesolimbic system is driven by dopamine release.
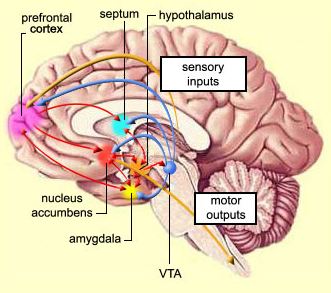 |
(c) The amygdala is localized in the temporal lobe, anterior to the hippocampus. Its activity appears related to emotions.
(d) the hippocampus and
(e) the bed nucleus of the stria terminalis. The stria terminalis is a major amygala output pathway.
 |
 |
 |
(2) the second system, the nigrostriatal pathway, describes neurons that project from the substantia nigra to the caudate and putamen; the system has been described in detail earlier as central to the pathogenesis of Parkinson's disease.
(3) the third pathway runs from the arcuate nuclei and periventricular neurons to the hypothalamus and posterior pituitary and constitutes the tuberoinfundibular system.
(4) the fourth has originating neurons in the motor nucleus of the vagus nerve but projections are not well characterized; the system is the medullary-periventricular pathway.
(5) connections between the medial zone inserted to the hypothalamus and amygdala described the incertohypothalamic system.
The principal idea is that above normal limbic dopaminergic activity is related in an important way to psychosis.136
The suggestion has been supported by several observations.
(1) One line of evidence is based on the strong antagonist properties of many antipsychotic agents at postsynaptic D2 CNS receptors, localized particularly in the mesolimbic and striatal-frontal cortex.
This observation extends to include some partial dopamine agonists such as aripiprazole (approved by the FDA for treatment of schizophrenia) and bifeprunox (an experimental agent not granted FDA approval), which exhibit both limited D2 receptor activation and 5-HT2 receptor blockade.
(2) Another line of evidence is that drugs that activate dopamine receptors such as the well-known examples of L-DOPA, bromocriptine, apomorphine, and amphetamines typically worsen schizophrenia psychosis and in some cases induce psychosis in patients previously not exhibiting them.
(3) Additionally, when dopamine-receptor concentration was determined postmortem in brains of schizophrenic patients who had not been treated with antipsychotic drugs, the receptor concentration was elevated.
(4) Also, in some postmortem studies, brains of schizophrenic patients exhibited both increased dopamine levels and D2 receptor density in caudate and putamen as well as in the nucleus accumbens.
(5) Lastly, amphetamine-induced striatal dopamine release, increased baseline striatal D2 receptor occupancy and other indications of increased striatal dopamine synthesis and release have been suggested by imaging studies.
Despite the above suggestions of elevated limbic dopaminergic activity being important in psychosis, other findings are more in line with diminished dopaminergic activity in these regions.136
For example, both postmortem and in vivo imaging studies of limbic, and striatal, nigral and cortical regions support the idea of reduced dopaminergic activity.
Also, reduced dopaminergic innervation in several sites, including dorsolateral prefrontal cortex, hippocampus, and medial temporal cortex along with reduced DOPAC (a dopamine metabolite) in the anterior cingulate have been found in postmortem studies.
These results would support diminished cortical or hippocampal dopaminergic activity associated with both cognitive impairment in schizophrenia negative symptoms.136
Along the same line, some of the "atypical" antipsychotic agents which are effective in management schizophrenia exhibit more limited effects at D2 receptor sites.
This observation emphasizes the importance of developing perhaps additional agents that affect multiple receptors, particularly serotonergic and glutaminergic systems.
The atypical antipsychotic agents often combine "weak" D2 receptor blockade with more substantial 5-HT2A receptor antagonism.136
![]()
|
|
|
|
|
|
|
|
| This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |