|
|
|
|
|
|
|
Medical Pharmacology Chapter 13 Opioids: Advanced Topics
|
|
|
|
|
|
|
1Intravenous Opioid Anesthetics: Cerebral Blood Flow
1Administration of other drugs/anesthetics influence the effect of opioids on cerebral blood flow.
However, opioids themselves slightly decrease cerebral metabolic rate by about 17% and decrease intracranial pressure (ICP).
In the context of vasodilation produced by inhalational agents, opioids they will produce cerebral vasoconstriction.
In the presence of nitrous oxide, opioids will diminish cerebral blood flow (CBF).
Cerebral blood flow is not affected substantially by opioids alone.
1,1tPositron emission tomography analysis
following fentanyl administration (1.5![]() g/kg,
IV) to human volunteers indicated that fentanyl effects on blood flow were
heterogeneous.
g/kg,
IV) to human volunteers indicated that fentanyl effects on blood flow were
heterogeneous.
For example, pain increased regional cerebral blood flow in the anterior cingulate, ipsilateral thalamus, prefrontal cortex, in contralateral supplementary motor area.
Fentanyl increased regional blood flow in the anterior cingulate in contralateral motor cortices but decreased the regional blood flow in the thalamus (bilateral effect) and posterior cingulate during both stimuli.
With pain stimulation as well as fentanyl administration, fentanyl appeared to augment pain-related regional blood flow increases in the supplementary motor area and prefrontal cortex.
This PET-based activation pattern accompanied decreased pain perception using the visual analogue scale.
This analysis indicated that fentanyl analgesia appeared to augment pain-evoked cerebral responses in some areas but activated and inhibited other brain regions that were not responding to pain stimulation by itself.
1For patients undergoing carotid artery surgery, CBF during fentanyl-nitrous oxide or isoflurane (0.75%)-nitrous oxide anesthesia was reduced relative to halothane (0.5%)-nitrous oxide anesthesia.
Furthermore, balanced anesthesia with fentanyl-nitrous oxide appeared to better maintain the cerebrovascular response to CO2 in those patients with an edematous brain relative to isoflurane-nitrous oxide anesthesia protocols.
1Sufentanil and fentanyl have been noted to
increase middle cerebral artery blood flow velocity by about 25%; other
clinical research indicated that in healthy human volunteers, sufentanil
(0.5 ![]() g/kg IV)
did not result in effect on CBF.
g/kg IV)
did not result in effect on CBF.
In a patient group consisting of those undergoing carotid endarterectomy, sufentanil 1.5-2.0-μg/kg bolus + 0.2-0.3-μg/kg/h infusion of-nitrous oxide anesthesia caused CBF effects comparable to that observed with isoflurane (0.75%)-nitrous oxide anesthesia with maintenance of CO2 cerebrovascular reactivity.
Alfentanil (25 or 50 μg/kg IV) given to patients who were receiving isoflurane (0.4-0.6%)-nitrous oxide anesthesia resulted in very small reductions in middle cerebral artery flow velocity.
CBF values during remifentanil-nitrous oxide anesthesia were reported similar to CBF values measured during fentanyl-nitrous oxide and isoflurane-nitrous oxide anesthesia, at the same time cerebrovascular reactivity to CO2 remained.
1Intravenous Opioid Anesthetics: Intracranial Pressure
Generally, opioids do not have significant effects on intracranial pressure (ICP).
For patients undergoing craniotomyfor supratentorial space-occupying tumors, opioids do not cause significant increases in ICP or CSF pressure (anesthesia was provided utilizing isoflurane-nitrous oxide).
ICP does not appear to be altered in head-injury patients who are receiving opioids sedation.
However, other research indicates that harmful opioid-induced ICP effects could be produced-- even in the context of patients undergoing craniotomy for supratentorial tumors with mass effect, opioids could increase ICP, perhaps particularly if intracranial compliance has been compromised by tumor dimensions.
Accordingly, the precise effect of opioid administration on intracranial pressure may vary depending on the precise clinical circumstance as well as on potentially the nature of the background anesthetic.
For certain brain tumor patients anesthetized with thiopental-nitrous oxide-vecuronium, following sufentanil (1 μg/kg) CSF pressure increased nearly twofold and increased by about 1.2X following alfentanil (50 μg/kg).
Comparable patients exhibit a reduction in CSF (5%) following fentanyl (5 μg/kg).
This last result has been verified by an additional worker with respect to fentanyl and alfentanil.
Again, on the other hand, other
studies reported no effect of alfentanil (70![]() g/kg
infused over 6 minutes) on ICP in hydrocephalic patients (age
range: 1.3-20
years) who were operated on for shunt revision under isoflurane
(0.5%)-nitrous oxide anesthesia.
g/kg
infused over 6 minutes) on ICP in hydrocephalic patients (age
range: 1.3-20
years) who were operated on for shunt revision under isoflurane
(0.5%)-nitrous oxide anesthesia.
Yet, in a different study results indicated that sufentanil (0.6 μg/kg) and fentanyl (3 μg/kg) administration caused significant increases in ICP in fully resuscitated individuals who had severe head trauma.
In reviewing all these studies, it appears difficult to predict the exact effect on opioids in any specific circumstance.
It is possible that inconsistent results could be due to differences in ICP or CSF pressure assessment methodologies, due to influences of other drugs present, or for reasons undetermined.
Consult the details in reference 1, if desired, for references to the primary literature, the results from some of which have been noted above).
The possible effects of opioids on ICP-focusing on increases in ICP may be due to direct cerebrovascular influences and/or more indirect effects secondary to changes in mean blood pressure or cerebral perfusion pressure with compensatory cerebral vasodilatation.
Which one of these possibilities is more likely true remains for future research to decide.
If ICP effects to the opioids were principally secondary to opioid-induced cardiovascular effects, then rapid management of such cardiovascular effects could reduce or prevent adverse ICP effects.
ICP increases could also be secondary to opioid-induced rigidity.
At least for fentanyl, CSF production rates and CSF reabsorption rates do not appear to be affected.
1Intravenous Opioid Anesthetics: Muscle Rigidity
1Increases in muscle tone and muscle rigidity may be associated with opioid administration.
Patients receiving dehydrobenzperiol (0.44 mg/kg) along with fentanyl (8.8 μg/kg) have a four out of five chance of exhibiting some rigidity.
A single IV fentanyl dose of 0.5-0.8 mg will reliably induce chest wall rigidity within about 60-90 seconds.
Variations in dosage and administration speed are probably responsible for differing incidence of rigidity.
Other factors that contribute to variability include whether or not nitrous oxide is used, the presence or absence of muscle relaxants in patients age.
2Relatively large doses of IV morphine ( 2 mg/kg infused at a rate of 10 mg/minute) induces abdominal muscle rigidity with reduced thoracic compliance.
The maximal effect under these circumstances is reached at about 10 minutes following administration.
Individuals receiving smaller morphine doses in the rate of 10-15 mg have recounted feelings of muscle tension usually in the neck or legs with occasional presentations around the chest.
Elaborating on the nitrous oxide effect noted above, muscle rigidity is significantly increased by 70% nitrous oxide.
Following high-dose opioids, myoclonus in the absence of the EEG evidence of seizure activity has also been noted.
2Muscle rigidity secondary to opioid administration appears to be a μ-receptor mediated activity at supraspinal sites such as the nucleus raphe pontis in addition to lateral proximal sites.
2Opioid-induced rigidity can be managed or eliminated by drugs such as naloxone as well as those agents which increased GABA agonist action including thiopental and diazepam and other muscle relaxants.
1Rigidity secondary to opioids may be described by increasing muscle tone which can progress to severe stiffness.
The clinically significant opioid-induced rigidity is usually first detectable just as or immediately after the patient loses consciousness.
In conscious patients relatively mild presentations of rigidity manifest as hoarseness.
The most frequent initial identifier of opioid rigidity is wrist flexion.
Time course of rigidity: occasionally rigidity can occur upon anesthesia emergence and less commonly hours following the last opioid dose administration.
These delayed or postoperative events are most likely explained by pharmacokinetic manifestations -- i.e. second peaks in plasma opioid concentrations.
1Pulmonary consequences:
Rigidity can cause a reduction in pulmonary compliance as well as reduced functional residual capacity.
Sometimes more importantly, opioid-induced rigidity may diminish or even prevent adequate ventilation resulting in hypercarbia, hypoxia with elevations in ICP.
1Cardiovascular consequences:
Opioid-induced rigidity changes in number of hemodynamic parameters-including causing an increase in pulmonary artery and central venous pressures as well as an increase in pulmonary vascular resistance.
Arterial blood pressure and cardiac output remained relatively constant.
![]() 1Abdominal and/or thoracic muscle rigidity
(wooden chest syndrome) was thought to be the reason for opioid-induced
impairment of spontaneous or controlled ventilation in the nonparalyzed
individual.
1Abdominal and/or thoracic muscle rigidity
(wooden chest syndrome) was thought to be the reason for opioid-induced
impairment of spontaneous or controlled ventilation in the nonparalyzed
individual.
Apparently, the difficulty in bag ventilation and masking following opioid administration is mostly due to vocal cord closure.
![]() 1More about the opioid induced rigidity
mechanisms:
1More about the opioid induced rigidity
mechanisms:
Opioid-induced rigidity is not to due to a direct action on muscle fibers; however the precise mechanism remains to be elucidated.
This conclusion follows from the observation that opioid-induced fiber rigidity can be prevented by pretreatment with muscle relaxants.
Furthermore, opioid-induced muscle rigidity is not accompanied by increases in creatinine kinase -- a result indicating that limited or no muscle damage occurs with rigidity.
From the electrophysiological point of view, opioids have limited effects on neuromuscular conduction depressing only minimally monosynaptic reflexes associated with muscle stretch receptors.
![]() -receptor
agonists as opposed to
-receptor
agonists as opposed to ![]() -or
-or ![]() -
agonists are effective in inducing rigidity (in the rat model).
-
agonists are effective in inducing rigidity (in the rat model).
Stimulation of GABA interneurons can result in a rigidity which can be blocked by stray lesions.
Striatonigral GABA pathways thought to be rigidity-related are influenced by GABA agonists and antagonists.
There has been some suggestion of relationships between basic neurochemical mechanisms that are involved in Parkinson's disease and opioid-induced catetonia and rigidity.
This consideration follows from the increase opioid-induced rigidity with age as well as muscle movement abnormalities similar to extrapyramidal side effects.
![]() 1More about management of opioid-induced
rigidity:
1More about management of opioid-induced
rigidity:
Rapid termination of opioid-induced rigidity follows from succinylcholine administration.
Succinylcholine also obviates associated cardiovascular changes and typically allows controlled ventilation.
Preventative measures are however considered more definitive in dealing with this problem.
Administration of nondepolarizing muscle relaxants reduces severity and incidence of rigidity.
Beyond this observation some inconsistency exists in the literature concerning other approaches.
For example thiopental induction doses with reduced relative to anesthetic doses of diazepam and midazolam may prevent, reduced, or effectively manage rigidity.
On the other hand, the reliability of benzodiazepines in this application has been questioned.
Opioid-induced rigidity may also be attenuated by
administration of ketanserin, amantadine, and
![]() 2-agonists.
2-agonists.
The best method to avoid rigidity in clinical practice appears to involve concomitant administration of a "priming" size dose of a nondepolarizing agent along with avoiding rapid large dose administration of any opioid.
The use of an "priming" dose of nondepolarizing agent is to avoid the possibility of muscle relaxation prior to unconsciousness.
Opioid-induced rigidity in the presence of apnea has been taken to indicate unconsciousness.
Anesthetists may choose to demonstrate the ability to mask ventilate the patient following anesthesia induction but prior to the administration of a muscle relaxant.
This approach will be of only questionable value should opioid-induced rigidity occur during induction, resulting in increased difficulty or even impossibility of patient ventilation.
In view of this observation, should a patient presents with a difficult airway, or the possibility of a difficult airway, or other circumstances exist requiring assurance of the patient must be/can be manually ventilated prior to neuromuscular blockade, as a consequence that only small opioid doses should be given during induction.
Efforts to mask ventilate a patient with opioid-induced muscle rigidity can result in gastric insufflation with inadequate ventilation and oxygenation pending administration and activity of muscle relaxant.
With large doses of opioids used, anticipation of the need for rapid neuromuscular blockade should be part of preoperative planning.
2Intravenous Opioid Anesthetics: Nausea and Vomiting
![]() Nausea and vomiting are significant side
effects of morphine and related compounds.
Nausea and vomiting are significant side
effects of morphine and related compounds.
Interoperative opioids as well as morphine premedication may be associated with increased incidence of postoperative vomiting.
This issue is particularly important in view of increasing prominence of same day surgical procedures and the observation that nausea and vomiting may predispose to an overnight stay.
Independent of the route of administration (oral, intravenous, intramuscular, transmucosal, subcutaneous, transdermal, intrathecal, epidural, or intramuscular) the likelihood of opioid-induced nausea turns out to be similar.
At least concerning morphine, meperidine, fentanyl, sufentanil, and alfentanil, the severity and incidence of nausea and vomiting appear similar through the series.
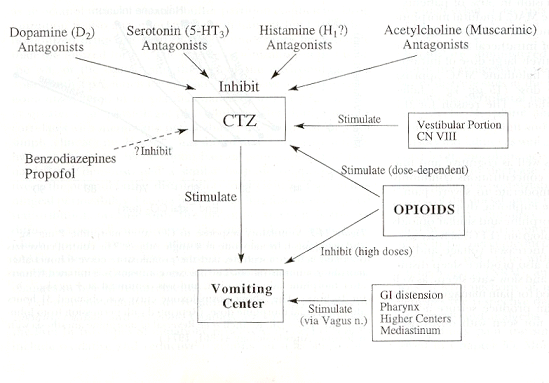
![]() Neuropharmacology of opioid-induced
nausea and vomiting is complex and is represented in the figure below:
Neuropharmacology of opioid-induced
nausea and vomiting is complex and is represented in the figure below:
|
|
2"The chemotactic trigger zone (CTZ) located in the area postrema the brainstem, contains dopamine, serotonin, histamine, and muscarinic acetylcholine is well as opioid receptors. The vomiting center receives input from the CTZ as well as peripheral sites via the vagus nerve. As illustrated, the role of opioids as complex, and they appear to have both emetic and antiemetic effects."
The vomiting center receives neuronal input from the chemotactic triggers on (CTZ) in the area postrema of the medulla, as well as from the pharynx, GI tract, mediastinum, and visual center.
The CTZ is associated with a number of receptor systems including opioid, dopamine (D2), serotonin (5-HT3), histamine, and acetylcholine (muscarinic).
The CTZ receives input from the vestibular portion of these cranial nerve. Increased vestibular sensitivity is associated with morphine administration and morphine as well as related opioids can cause nausea by direct CTZ stimulation.
Morphine's nausea and emetic effects are increased by vestibular stimulation which can accompany walking, for example.
At the vomiting center, higher morphine (and other opioid) doses exhibits an antiemetic effect which is naloxone-reversible.
The antiemetic effect does not appear to last as long as emetic action of morphine.
The results of an experiment which demonstrated this relationship indicated that morphine-induced nausea and vomiting tended to increase when a morphine infusion was discontinued. (Another possibility was noted -- accumulation of the active morphine metabolite, morphine-6-glucuronide continue to accumulate throughout this period which resulted in a worsening of nausea.)
Treatment of opioid induced nausea and vomiting (and prophylaxis) has involved administration of other medications which are antagonists at a number of the receptor sites in the CTZ.
Some antiemetic agents have not had their mechanisms elucidated; some of these agents include benzodiazepines and propofol.
(The Digital Slice of Life is a cooperative project with the Slice of Life office, KUED Media Solutions, and the Knowledge Weavers Project.) )
|
|
|
|
|
|
|
DISCLAIMER
|
1Bailey, PL, Egan, TD, Stanley, TH, "Intravenous Opioid Anesthetics", in Anesthesia 5th edition, Miller, R.D., editor, Churchill Livingstone, Philadelphia, 2000, 273-377 (references secondarily sourced from this primary reference are noted below in the indented references)
1aLowenstein, E, Hallowell P, Levine FH et al.: Cardiovascular response to large doses of intravenous morphine in man.N. Engl J Med 281:13 89, 1969
1b Stanley, TH, Webster LR; Anesthetic requirements and cardiovascular effects of fentanyl-oxygen and fentanyl-diazepam-oxygen anesthesia in man. Anesth Analg 51:901, 1972.
1c Arens, JR, Benbow, BP, Ochsner JL et al: Morphine anesthesia for the aorto-coronary bypass procedures. Anesth Analg 57: 411, 1978
1d Stanley, TH, Gray NJ, Staford W. et al: The effects of high-dose morphine on fluid and blood requirements in open-heart operations. Anesthesiology 38:536, 1973.
1e Stoelting, RK, Gibbs PS, Creasser CW et al: Hemodynamic in ventilatory response to fentanyl, fentanyl-droperidol, and nitrous oxide in patients with acquired valvular heart disease. Anesthesiology 42:319, 1975.
1f Bowdle, TA, Ward, RJ: Induction of anesthesia with small doses of sufentanil or fentanyl: Dose versus EEG response, speed of onset and thiopental requirement. Anesthesiology 70:26, 1989
1gHecker BR, Lake CL, DiFazio CA et al: The decrease of the minimum alveolar anesthetic concentration produced by sufentanil in rats. Anesth Anal 62:987, 1983.
1hGoldstein,A: Opiate receptors. Life Sci. 14:615, 1974.
1iSnyder SH: Opiate receptors in the brain. N Engl. J Med to 96:266, 1977.
1jMayer, DJ, Wolfle, TL, Akil H et al: Analgesia from electrical stimulation in the brainstem of the rat. Science 174:13 51, 1971.
1kFields, HL: Brainstem mechanisms of pain modulation: Anatomy and physiology. In Herz, A (ed): Opioids II: Handbook of Experimental Pharmacology. Berlin, Springer-Verlag, 1993, p.3.
1lKissin I, Vinik HR, Castillo R et al:Alfentanil potentiates midazolam-induced unconsciousness in subanalgesic doses. Anesth Analg 71:65, 1990
1mMcEwan AI, Smith C, Dyar O et al: Isoflurane minimum alveolar concentration reduction by fentanyl. Anesthesiology 78:864, 1993.
1nBailey, PL, Wilbrink J, Zwanikken P et al: in Anesthetic induction with fentanyl. Anesth. Analg 64:45, 1985.
1oHeier, T, Steen, PA: Assessment of anesthesia depth.Acta Anaesthesiol Scand 40:10 87, 1996.
1pSebel PS Lang E Rampil IJ White PF Cork R Jopling M Smith NT Glass PSA Manberg A multicenter study of bispectral electroencephalogram analysis for monitoring anesthetic effect Anesth. Analg. 84(4) 1997 891-899.
1qJones, JG: Use of evoked responses in the EEG to measure depth of anesthesia. In Lunn J, Rosen M (eds): Consciousness, Awareness and Pain and General Anesthesia. Boston, Butterworth, 1987, p 99.
1rEgan TD, Minto CF, Hermann DJ et al: Remifentanil versus alfentanil: Comparative pharmacokinetics and pharmacodynamics. Anesthesiology 84: 821, 1996.
1sKalkman CJ, Rheineck AR, Bovill JG: of high-does opioid anesthesia on posterior tibial nerve somatosensory cortical evoked potentials: Effects of fentanyl, sufentanil, and alfentanil J Cardiothorrac Anesth 2:758, 1998.
1tAdler, LJ, Fyuulai F, Diehl D, Mintun, M, Winter, PM, Firestone, L Regional brain activity changes associated with fentanyl analgesia elucidated by positron emission tomography. Anesth Analg 1997; 84:120-126.
2Coda, BA, "Opioids" in Clinical Anesthesia, 4th edition, Barash, PG, Cullen, BF, Stoelting, RK, editors, Lipincott Williams and Wilkins, Philadelphia, 2001, 345-375
2a Thorpe, DH: Opiate structures and activity: a guide to underlying opioid actions. Anesth Analg 63:143, 1984.
3Gottschalk, A and Smith DS, New Concepts in Acute Pain Therapy: Preemptive Analgesia, American Family Physician, May, 2001 http://www.aafp.org/afp/20010515/1979.html
First figure redrawn with permission by Gottschalk and Smith from: Kehlet H, Dahl JB. The value of "multimodal" or "balanced analgesia" in postoperative pain treatment. Anesth Analg 1993;77:1049.
Second figure redrawn with permission by Gottschalk and Smith from: Woolf CJ, Chong MS. Preemptive analgesia--treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg 1993;77:368.
4Dickenson, AH Spinal cord pharmacology of pain. Br. J. Anaesth. 75: 193, 1995. (references secondarily sourced from this primary reference are noted below in the indented references)
4aBattaglia, G, Rustioni A. Coexistence of glutamate and substance P. and dorsal root ganglion cells of the rat and monkey. Journal of Comparative Neurology 1988; 277:302-312.
4bHaley, JE, Sullivan, AF, Dickenson, AH. Evidence for spinal N-methyl-D-aspartate receptor involvement in prolonged chemical nociception in the rent. Brain Research 1990; 518:218-222.
4cSchiable, HG, Grubb BD, Neugebauer, V, Oppmann M. The effects of NMDA antagonists on neuronal activity in cat spinal cord evoked by acute inflammation in the knee joint. European Journal of Neuroscience, 1991; 3:981-991.
4dWoolf CJ, Thompson, SWN. The induction and maintenance of central sensitization is dependent on N--methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury hypersensitivity states. Pain 1991; 44:293-299.
4eMao, J, Price DD, Hayes, RL, Lu, J, Mayer DJ, Frank H. Intrathecal treatment with dextrophan or ketamine publicly reduces pain-related behaviors in a rat model of peripheral mononeuropathy. Brain Research 1993; 605:164-168.
4fPrice, DD, Mao, J, Mayer DJ. Central neural mechanisms of normal in abnormal pain states. In: Fields, HL, Lebeskind, JC, eds. Progress in Pain Research and Management. Seattle:IASP Press, 1994; 61-84.
4gRogawaki MA. Therapeutic potential of excitatory amino acid antagonists; channel blocks and 2,3 benzodiazepines. Trends in Pharmacological Sciences 1993; 14:325-331
4hEide PK, Jorum E, Stubhaug, A, Bremnes J, Breivik H. Relief of post-herpetic neuralgia with the N-methyl-D-aspartate receptor antagonist ketamine: a double-blind, cross-over comparison with morphine and placebo. Pain 1994; 58:347-354.
4iPrice DD, Mao J, Frenk H, Mayer, DF. Central neural mechanisms of normal in abnormal pain states. In:Fields HL, Lebeskind JC, eds. Progress in Pain Research and Management. Seattle:IASP Press, 1994; 61-84.
4jBesse, D, Lomabard, MC, Zajac, JM, Roques, BP, Besson, JM Pre- and and postsynaptic distribution of mu, delta, and kappa opioid receptors in the superficial layers of the cervical dorsal horn of the rat spinal cord, Brain Research 521 (1-2), June 1990 pp 15-22.
4kKangrga I and Randic M Outflow of endogenous aspartate in glutamate from the rat spinal dorsal horn in vitro by activation of low-and high-threshold primary afferent fibers. Modulation by mu-opioids Brain research 553, 2, July 1991,pp. 347-352.
5Substantia Gelatinosa Image: Courtesy of
The Digital Slice of Life, a cooperative project with the Slice
of Life office, KUED
Media Solutions, and the Knowledge
Weavers Project.
Ross, AF, Gomez, MK, Tinker, JH "Anesthesia for Adult
Cardiac Procedures in Principles and Practice of Anesthesiology, 2nd
edition, Longnecker, DE, Tinker, JH, Morgan, GE, eds, Mosby, St. Louis,
1998, pp. 1659-1698.
6Two-dimensional and Three Dimensional Images courtesy of CORD Center for Opioid Research and Design http://www.opioid.umn.edu/
7Jaffe, CC, Stewart, WB, Lynch, PJ, Hines, S., Cranial Nerves, Yale University School of Medicine, Center for Advanced Instructional media, (c) 1998 http://info.med.yale.edu/caim/cnerves/contents.html
8Kauffman, AM and Patel M, Center for Cranial Nerve Disorders http://www.umanitoba.ca/cranial_nerves/trigeminal_neuralgia/manuscript/index.html
9Chakrabarti, S, Oppermann, M Gintzler AR Chronic morphine induces the concomitant phosphorylation and altered Association of multiple signaling proteins: A novel mechanism for modulating cell signaling PNAS 98 (7) 4009, 2001
10Brookoff, D Chronic Pain: 1. A New Disease? Hospital Practice July, 2000 http://www.hosppract.com/issues/2000/07/brook.htm
11Protein Structure Study Guide http://www.princeton.edu/~actin/chm543_info.html#Study%20guide%201
12MRC Center for Synaptic Plasticity, University of Bristol, used with permission for non-commercial applications
13Breeze AL, Harvey, TS, Bazzo, R, Campbell ID Solution structure of Human Calcitonin Gene-Related Peptide by H NMR and Distance Geometry with Restrained Molecular Dynamics Biochemistry 30:575-582 (1991)
14Heish, JC, Carr, DB "Choosing a Therapeutic Approach: Opioids" in The Massachusetts General Hospital Handbook of Pain Management (Borsook D, LeBel, AA, McPeek, B, eds) Little, Brown and Company, Boston, 1996, pp 47-75.
15Anwari, J. S. and Iqbal, S. (2003)Antihistamines and potentiation of opioid induced sedation and respiratory depression. Anaesthesia 58 (5), 494-495
3aGustafsson LL, Schildt B, Jacobsen KJ. Adverse effects of extradural and intrathecal opiates: Reports of a nationwide survey in Sweden. British Journal of Anaesthesia 1982; 54:479-486.
3bBrockways MS, Nobel DW, Sharwood-smith GH, McClure JH. Are found respiratory depression after extradural fentanyl. British Journal of Anaesthesia 1990; 64:243-245.
3cHolmstrom, B, Rawal N, Axelsson K, Nydahl P. Risk of catheter migration during combined spinal epidural block. Percutaneous epiduroscopy study. Anesthesia and Analgesia 1995; 80:747-753.
16Yli-Hankala,A Will enough isoflurane during surgery replace morphine after surgery? Acta Anaesthesiologica Scandinavica Volume 47 Issue 7 Page 785 - August 2003)
17Gurman GM, Weksler N, Steiner O, Popescu M, Avinoah E, Porath A. The influence of cortical electrical activity level during general anaesthesia on the severity of immediate postoperative pain in the morbidly obese. Acta Anaesthesiol Scand 2003; 47:804-8
17Soliman E Legatt, AD Somatosensory Evoked Potentials: General Principles eMedicine, http://www.emedicine.com/neuro/topic640.htm, 8/2001.
18Black,
S, Sloan T., SOMATOSENSORY (SSEP) AND MOTOR EVOKED POTENTIALS (MEP) THE
SOCIETY FOR NEUROANESTHESIA AND CRITICAL CARE - 1998 ANNUAL MEETING http://analgesic.anest.ufl.edu/anest2/mahla/snacc/eps/