|
|
|
|
|
Nursing Pharmacology Chapter 8: Antiarrhythmic Agents
|
|
|
|
|
|
|
![]() Transmembrane potential --
determined primarily by three ionic gradients:
Transmembrane potential --
determined primarily by three ionic gradients:
Na+, K+, Ca 2+
Water-soluble and not free to diffuse through the membrane in response to concentration or electrical gradients: Transport is dependent upon membrane channel protein state.
Movement through channels depend on controlling "molecular gates"
Gate-status controlled by:
Ionic conditions
Metabolic conditions
Transmembrane voltage
Maintenance of ionic gradients:
Na+/K+ ATPase pump
Termed "electrogenic" when net current flows as a result of transport (e.g., three Na+ exchange for two K+ ions)
Initial permeability state associated with the resting membrane potential
Sodium: relatively impermeable
Potassium: relatively permeable
Cardiac cell permeability and conductance:
Conductance: determined by characteristics of ion channel protein
Current flow = voltage X conductance
Voltage = (actual membrane potential - membrane potential at which no current would flow, even with channels open)
Concentration gradient: 140 mmol/L Na+ outside: 10 mmol/L Na+ inside;
Electrical gradient: 0 mV outside; -90 mV inside
Driving force -- both electrical and concentration -- tending to move Na+ into the cell.
In the resting state: sodium ion channels are closed therefore no Na+ flow through the membrane
In the active state: channels open causing a large influx of sodium which accounts for phase 0 depolarization.
|
|
|
Concentration gradient (140 mmol/L K+ inside; 4 mmol/L K+outside)
Concentration gradient -- tends to drive potassium out
Electrical gradient tends to hold K+ in.
Some K+ channels ("inward rectifier") are open in the resting state -- however, little K+ current flows because of the balance between the K+ concentration and membrane electrical gradients
Cardiac resting membrane potential: mainly determined
By the extracellular potassium concentration and
Inward rectifier channel state
Spontaneous Depolarization (pacemaker cells)-- phase 4 depolarization
Spontaneous Depolarization occurs because:
Gradual increase in depolarizing currents (increasing membrane permeability to sodium or calcium)
Decrease in repolarizing potassium currents (decreasing membrane potassium permeability)
Both factors are important.
Ectopic pacemaker: (not normal SA nodal pacemakers) --
Facilitated by hypokalemic states
Increasing potassium: tends to slow or stop ectopic pacemaker activity
Depolarization to threshold voltage--Na+
m gate activation (activation gate); assuming inactivation (h) gates are not closed then
Sodium permeability dramatically increased; intense sodium current
Depolarization
h gate closure; Na+ current inactivation
|
|
|
|
|
|
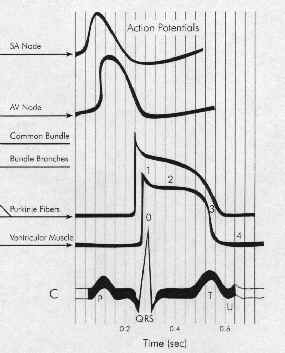
Five Phases: cardiac action potential associated with HIS-purkinje fibers or ventricular muscle
Phase 0 corresponds to Na+ channel activation.
The maximum upstroke slope of phase 0 is proportional to the sodium current.
Phase 0 slope is related to the conduction velocity in that the more rapid the rate of depolarization the greater the rate of impulse propagation.
Phase 1 corresponds to an early repolarizing K+ current.
Rapidly inactivated.
Phase 2 is the combination of an inward, depolarizing Ca2+ current balanced by an outward, repolarizing K+ current (delayed rectifier).
Phase 3 is also the combination of Ca2+ and K+ currents.
Phase 3 is repolarizing because the outward (repolarizing) K+ current increases while the inward (depolarizing) Ca2+ current is decreasing.
Phase 4 in normal His-Purkinje and ventricular muscle cells is characterized by a balance between outward Na+ current and inward K+ current.
As a result, the resting membrane potential would normally be flat.
In disease states or for other cell types (SA nodal cells) the membrane potential drifts towards threshold.
This phenomenon of spontaneous depolarization is termed automaticity and has an important role in arrhythmogenesis.
Hondeghem, L.M. and Roden, D.M., "Agents Used in Cardiac Arrhythmias", in Basic and Clinical Pharmacology, Katzung, B.G., editor, Appleton and Lange, 1998, pp 216-241.
|
|
|
|
|
|
|