|
|
|
|
|
|
|
Nursing Pharmacology Chapter 33-34: Anticancer Drugs
|
|
|
|
|
|
|
Natural Products:
Topoisomerase Inhibitors Type II: Mitoxantrone (Novantrone) (mye toe ZAN trone)
|
|
|
|
|
![]() Mitoxantrone
was shown to be the most active of the anthracenediones, synthesized in the
1970s and exhibited antitumor activity in murine leukemia models.8
Mitoxantrone
was shown to be the most active of the anthracenediones, synthesized in the
1970s and exhibited antitumor activity in murine leukemia models.8
Early on, in both preclinical and clinical studies, differences between mitoxantrone and the anthracyclines were noted not only in terms of mechanism of action with reduced cardiotoxicity but also with respect to other adverse effects.
The range of antitumor mitoxantrone activity appears comparatively narrow, explaining its use mainly in prostate cancer treatment, leukemias and lymphomas and explaining limited replacement by mitoxantrone for doxorubicin in the clinical setting.8
![]() Mitoxantrone (Novantrone)
is FDA approved for treating advanced hormone-refractory prostate malignancy
and acute myeloid leukemia (AML) as well as "late-stage, secondary
progressive multiple sclerosis."1,7
Mitoxantrone (Novantrone)
is FDA approved for treating advanced hormone-refractory prostate malignancy
and acute myeloid leukemia (AML) as well as "late-stage, secondary
progressive multiple sclerosis."1,7
Mitoxantrone in the context of multiple sclerosis is limited to treatment of secondary or chronic "progressive, progressive relapsing, or worsening or relapsing-remitting multiple sclerosis." 9
The intent of mitoxantrone administration is the reduction of neurologic disability and/or a reduction in the frequency of relapse.9
Mitoxantrone also appears useful in treating low-grade non-Hodgkin's lymphoma and breast cancer.3
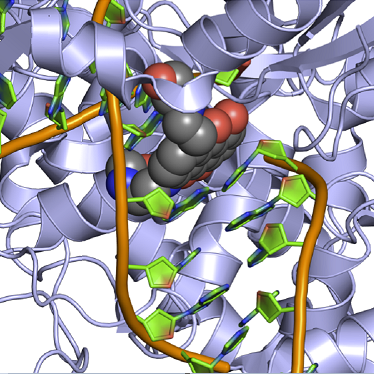
Mitoxantrone exhibits a similar mechanism of action compared to anthracyclines in that mitoxantrone intercalates into DNA.9
|
|
|
A consequence of intercalation is cross-linking and strand breakage.
![]() Binding to
nucleic acids, mitoxantrone inhibits both DNA and RNA synthesis through
disordering the template and through steric effects.
Binding to
nucleic acids, mitoxantrone inhibits both DNA and RNA synthesis through
disordering the template and through steric effects.
Binding to DNA polymerase II, mitoxantrone decreases replication and also may inhibit incorporation of uridine into RNA and thymidine into DNA.
Mitoxantrone is classified as a non-cell-cycle-specific agent, biologically active at all cell-cycle stages.9
![]() Mitoxantrone is
classified as a anthracenedione, lacking the amino sugar found in
anthracyclines.10
Mitoxantrone is
classified as a anthracenedione, lacking the amino sugar found in
anthracyclines.10
This agent was developed in part as a non-cardiotoxic anthracycline-related drug.
Mitoxantrone administration may result in congestive cardiomyopathy, but at a lower incidence compared to doxorubicin.
Incidence of clinically relevant congestive heart failure is <2%.
![]() Previous
treatment with doxorubicin increases the likelihood of mitoxantrone
cardiotoxicity.10
Previous
treatment with doxorubicin increases the likelihood of mitoxantrone
cardiotoxicity.10
Absorption, Distribution, Biotransformation, Excretion:
Mitoxantrone is administered by the intravenous (IV) route of administration.9
This drug is distributed extensively in tissue but appears not to cross the blood-brain barrier.9
Mitoxantrone volume of distribution (Vd) is >1000 L/m2.
Mitoxantrone binds significantly to plasma proteins (80%).9
In humans, mitoxantrone pharmacokinetics (plasma concentration-time curve) appears best represented by 3-compartment model.11
A short absorption half-life is estimated between 4-10 minutes with the distribution phase extending from about 0.5 hours to 3 hours.
Considerable variability is been reported for the terminal half-life (9 hours-9 days).
The large volume of distribution suggest mitoxantrone sequestration in deep tissue compartments.
The major route of elimination mitoxantrone is bile with reduced amounts excreted by the urine.
The primary dose-limiting toxicity for mitoxantrone is myelosuppression with leukopenia.
Also observed adverse reactions include mild nausea and vomiting, alopecia, and mucositis.
1-2 days following mitoxantrone administration, blue discoloration of sclera, fingernails and urine is noted.
Mitoxantrone (Novantrone) is FDA approved for treating advanced hormone-refractory prostate malignancy and acute myeloid leukemia (AML) as well as "late-stage, secondary progressive multiple sclerosis."1,7
Mitoxantrone also appears useful in treating low-grade non-Hodgkin's lymphoma and breast cancer.3
|
|
|
|
|
|
|