|
|
|
|
|
|
|
Nursing Pharmacology Chapter 33-34: Anticancer Drugs
|
|
|
|
|
|
|
Natural Products:
Topoisomerase Inhibitors Type II: Epipodophyllotoxins: Teniposide (Vumon)
|
|
Teniposide (Vumon), like etoposide, complexes with DNA and topoisomerase II.
This ternary form (teniposide + topoisomerase II + DNA) inhibits resealing cleavage associated with topoisomerase action on DNA.1
![]() Broken DNA
strands accumulate, ultimately causing cell death.
Broken DNA
strands accumulate, ultimately causing cell death.
Of the cell-cycle phases, teniposide and etoposide are most effective in the S and G2 phases.1,9
Resistance to the action of etoposide and teniposide appear related to:1
(1) MDR1 gene amplification (Multi-Drug Resistance 1 gene)
(2) reduced topoisomerase II expression (or topoisomerase II mutation)
(3) p53 tumor suppressor gene mutation, limiting programmed cell death (apoptosis).1
![]() Teniposide has
limited clinical application but find some use in several cancers (used
along with anthracyclines and antimetabolites), such as:8
Teniposide has
limited clinical application but find some use in several cancers (used
along with anthracyclines and antimetabolites), such as:8
Neuroblastoma
Pediatric acute myelogenous leukemia (AML) (salvage treatment)
Childhood acute lymphoblastic leukemia (ALL) and
Lymphomas (salvage treatment)8
Absorption, Distribution, Biotransformation, Excretion:
Teniposide administration proceeds by the intravenous route.1
An initial more rapid redistribution from plasma exhibits a t1/2 of about 4 hours.
An extended distribution phase ensues with a t1/2 ranging from 10-40 hours.
About 44% of the agent is found in the urine in the form of metabolites (80%).1,9
Protein binding is substantial, >99% to albumin.
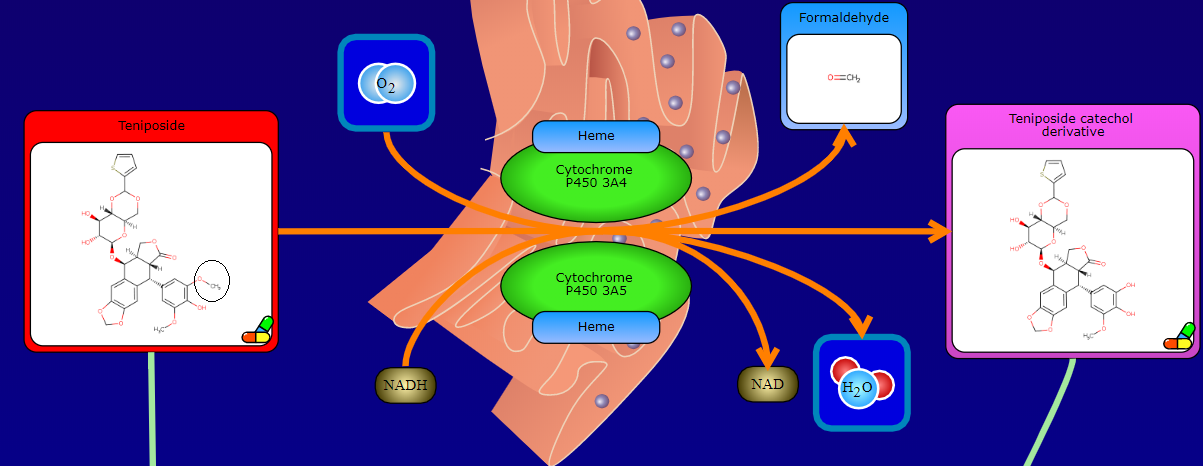
Hepatic metabolism dominates utilizing the cytochrome P450 microsomal metabolizing system, primarily the CYP3A4/5 isoforms.9,12 .
Teniposide is metabolized to catechol in the liver and to O-quinone in lysosomes.13
Some drugs that increase hepatic metabolism of teniposide include some anticonvulsants, such as phenytoin.1
As a consequence, systemic teniposide levels would be likely reduced.
Teniposide volume of distribution (Vd) ranges from about 3 to 11 L/m2 in children and about 8-44 L/m2 in adults.9
Distribution proceeds readily deliver, kidneys, small intestine but the drug has limited access to the CSF (<1%).9
|
|
The primary dose-limiting teniposide toxicity is myelosuppression (comparable to etoposide).
Other toxicities are often gastrointestinal such as vomiting, diarrhea as well as mild-moderate nausea.
Other side effects include alopecia and a late-occurring secondary leukemia.
There appears to be a greater likelihood of "hypersensitivity reactions" associated with teniposide administration compared to etoposide.7
Teniposide has limited clinical application but find some use in several cancers (used along with anthracyclines and antimetabolites), such as:8
Neuroblastoma
Pediatric acute myelogenous leukemia (AML) (salvage treatment)
Childhood acute lymphoblastic leukemia (ALL) and
Lymphomas (salvage treatment)8
Teniposide has been FDA approved for use in refractory acute info leukemia in the pediatric setting.7
|
|
|
|
|
|
|