|
|
|
|
Medical Pharmacology Chapter 35 Antibacterial Drugs
|
|
|
|
|
|
|
Sulfonamides
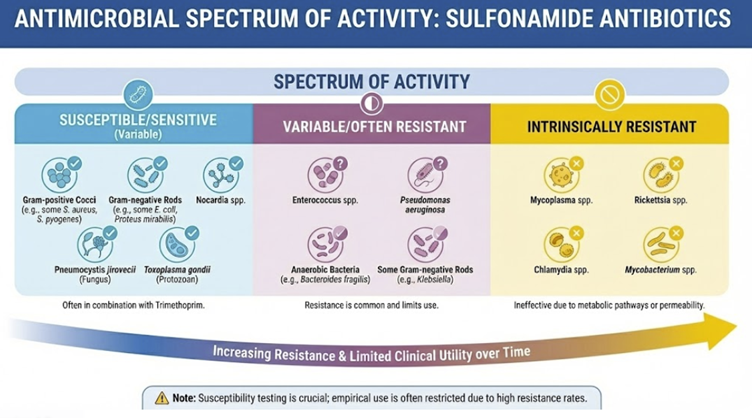 |
Antimicrobial Spectrum of Activity
Gram-Positive Bacteria
Activity includes Staphylococcus aureus,
including many community-associated methicillin-resistant S.
aureus (CA-MRSA) strains, Streptococcus pneumoniae,
and Streptococcus pyogenes.
The spectrum covers many common enteric and respiratory pathogens, including Escherichia coli, Klebsiella species, Proteus mirabilis, Shigella species, Vibrio species, and Haemophilus influenzae.
TMP/SMX (Trimethoprim/Sulfamethoxazole) is
active against Nocardia species and Listeria
monocytogenes. TMP/SMX may be effective against
Actinomyces species but is not the agent of first-choice
compared to tetracylines and carbapenems
The combination is highly effective against
several non-bacterial pathogens, including the protozoa
Toxoplasma gondii (Pyrimethamine is likely the most
effective agent against toxoplasmosis, used in combination with
other agents such as clindamycin or sulfadiazine),
Cystoisospora, and Cyclospora, and is the cornerstone
of therapy for the fungus Pneumocystis jirovecii.
Pharmacokinetics (Absorption, Distribution, Metabolism, Excretion (ADME))
Absorption
Most sulfonamides intended for systemic use are well-absorbed from the GI tract. Oral sulfonamides (e.g. sulfamethoxazole, sulfisoxazole, sulfadiazine) have bioavailability typically in the 70-100% range.6
Absorption occurs in the stomach and small intestine, and peak plasma levels are reached in 2-4 hours.6
Peak plasma levels occur about 1-4 hours after oral administration ; Cmax at steady state ranges from 57-68 µg/ml. 6
Some older sulfonamides with certain substitutions (e.g. sulfathalidine8, succinylsulfathiazole7) are poorly absorbed by design, so that they remain in the bowel.
These drugs were used for intestinal infections or bowel flora suppression.
Topical sulfonamides (ophthalmic drops, burn creams) can be absorbed through mucosa or damaged skin and may achieve systemic levels.9
Distribution
Sulfonamides distribute widely into body tissues and fluids.
They are relatively small molecules and, in their un-ionized form, cross cell membranes readily.
Sulfonamides achieve near-equivalent concentrations in pleural, peritoneal, synovial fluids, etc., compared to plasma.10
Sulfonamides also penetrate well into the cerebrospinal fluid (CSF) – levels in CSF can reach ~25-80% of plasma levels for various agents.11
For example, sulfadiazine is known to attain high enough levels in CSF to treat Toxoplasma encephalitis.
Sulfonamides also cross the placenta freely and enter fetal circulation12, and are excreted into breast milk.13
Sulfadiazine is considered by the manufacturer contraindicated in breast-feeding women.13
Binding to plasma proteins (primarily albumin) varies by agent and influences distribution and free drug levels.
Protein binding also underlies certain drug interactions and the risk of bilirubin displacement in neonates.14
Metabolism
Sulfonamides are metabolized chiefly in the liver, primarily by N-acetylation of the N4-amino group, and to a lesser extent by glucuronidation.
The acetylated metabolites have no antibacterial activity but may have increased propensity to precipitate in urine (acetyl-sulfonamides are less soluble).16
Sulfonamides crystallization in acidic urine was a serious issue, mitigated by using more soluble analogs and advising adequate hydration and urine alkalinization.17
The major modern sulfonamide, sulfamethoxazole, is partly metabolized by the cytochrome P450 system (notably CYP2C9 and CYP3A4).
Sulfamethoxazole is also an inhibitor of CYP2C9, which contributes to certain drug interactions (e.g. warfarin).18,19
Excretion
Most sulfonamides (and their metabolites) are primarily excreted by the kidneys. They undergo glomerular filtration and also tubular secretion.21
There is also some tubular reabsorption, especially for more lipid-soluble drugs, so half-lives can be prolonged in renal impairment.20
Urinary excretion is pH-dependent: alkalinization of urine increases excretion by keeping the drug ionized (and also helps prevent crystal formation).20
The plasma half-lives of sulfonamides vary widely from ~6 hours to >100 hours, which forms the basis for classifying them as short-, intermediate-, or long-acting.11
For instance, sulfisoxazole is eliminated quickly (t½ ~5–6 h), sulfamethoxazole intermediate (~11 h), sulfadiazine (~17 h), whereas sulfadoxine is extremely long-acting (~100–200 h)11,22
Because of renal elimination, doses must be adjusted in patients with renal insufficiency to avoid accumulation.23
In the elderly or those with reduced GFR, elimination is slower.
Sulfonamides readily cross the placenta and fetal elimination is inefficient (fetal acetylation), so the drug can accumulate in the fetus which has implications for toxicity (kernicterus) in late pregnancy and neonates.24
July, 2025
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |