|
|
|
|
|
|
|
Medical Pharmacology Chapter 35 Antibacterial Drugs
|
|
|
|
|
|
|
Penicillin G and Penicillin V Pharmacology and Therapeutics
Pharmacokinetics: Absorption, Distribution, Metabolism, Excretion (ADME)
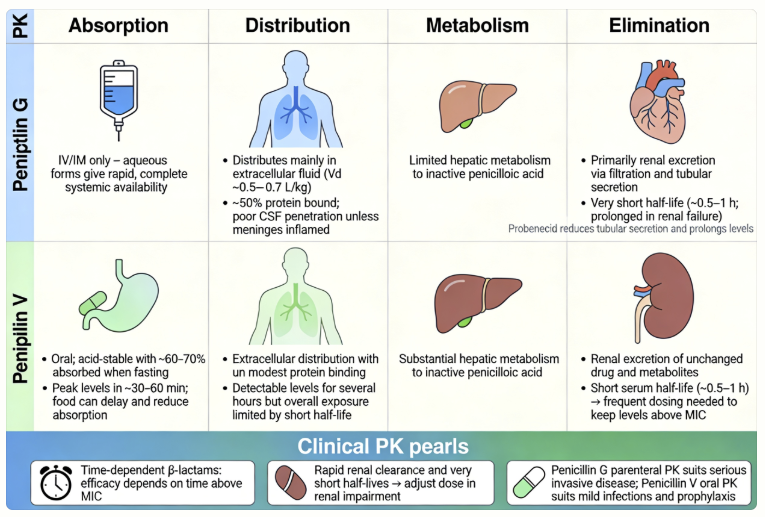 |
Absorption
The single most important pharmacokinetic difference between the two natural penicillins is their stability in gastric acid.
Penicillin G is acid-labile and is largely destroyed in the
acidic environment of the stomach, precluding its use as an oral
agent.
In
contrast, the phenoxymethyl side chain of penicillin V confers
acid stability, allowing it to survive passage through the
stomach and be absorbed in the small intestine.2
By
creating less soluble salts of penicillin G with
large organic molecules, intramuscular injected
drugs act as a reservoir, slowly releasing the
active drug over time
Administered intravenously, it provides
rapid, high peak concentrations, making
it ideal for treating severe, acute
infections in a hospital setting where
continuous or frequent dosing (e.g.,
every 4-6 hours) is feasible and high
drug levels are necessary
The procaine salt is more slowly
absorbed from the IM depot, maintaining
therapeutic concentrations for about 12
to 24 hours.
This approach allows for once- or
twice-daily dosing, suitable for
moderately severe infections that can be
managed on an outpatient basis or as
step-down therapy from IV treatment.
A single injection can provide
continuous, albeit very low, therapeutic
concentrations for up to four weeks.
![]() This
administration profile is suited for
eradicating highly sensitive organisms
where prolonged, uninterrupted exposure
is more critical than high peak
concentrations.
This
administration profile is suited for
eradicating highly sensitive organisms
where prolonged, uninterrupted exposure
is more critical than high peak
concentrations.
A notable example of this administration method is n the treatment of syphilis (Treponema pallidum).6,8,9
 |
|
Distribution
Once absorbed, both penicillins distribute into body fluids and tissues.
Penicillin V is more highly bound to plasma proteins
(approximately 80%) compared to penicillin G (approximately
60%).
Penicillins do not readily cross the blood-brain barrier in
healthy individuals.
Similarly, concentrations in synovial and peritoneal fluids are
higher during active inflammation
Penicillin G/V are handled as unchanged drugs. A limited amount of penicillin G undergoes hepatic metabolism to the inactive metabolite, penicilloic acid.2,4
Penicilloic acid is the major metabolite and is responsible for penicillin’s hapten formation leading to allergic reactions.10
Trace amounts of 6-aminopenicillanic acid (the core penicillin structure) and minor metabolites are also recovered in urine.4
Penicillin V undergoes metabolism in the range of 35%-70% of an oral dose metabolized to penicilloic acid.11
Penicillin effects on cytochrome P450 enzymes are typically quite limited and are unlikely to produce clinically relevant drug-drug interactions.12
Excretion
The kidneys are the principal route of elimination for both penicillin G and V.
Penicillins are excreted rapidly in urine via a combination of glomerular filtration and primarily active tubular secretion in the proximal tubules.4
About 60–90% of an IM dose of penicillin G is eliminated in the urine within the first hour due to efficient tubular secretion.
The plasma half-life of penicillin G in adults with normal renal function is only about 30–60 minutes3,4
Penicillin V’s half-life is similarly short (on the order of 30 minutes to 1 hour), necessitating dosing four times daily for oral penicillin V to maintain therapeutic levels.13
Because of this very rapid clearance, frequent dosing or continuous IV infusions are used for serious infections to keep levels above the minimum inhibitory concentration (MIC).13
Probenecid, a uricosuric drug, prolongs penicillin levels by competing for the same organic anion transporter (OAT) in the renal tubule, thereby blocking penicillin’s secretion.13
Co-administering probenecid can increase penicillin AUC and was used in the past to stretch limited penicillin supplies.13
Probenecid is sometimes employed to maintain high penicillin concentrations in severe infections like neurosyphilis or endocarditis.14,15
A smaller portion of penicillin elimination is non-renal: a fraction is cleared via biliary excretion, and minor metabolism contributes as noted.4 In renal impairment, penicillin’s clearance is reduced and dosage or interval should be adjusted to avoid accumulation (which could increase risk of se
In summary, the pharmacokinetics of penicillin G and V are characterized by rapid absorption (for acid-stable forms), wide distribution, minimal metabolism, and rapid renal excretion, making them very effective in appropriate clinical settings.
August, 2025
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |