|
|
|
|
|
|
|
Medical Pharmacology Chapter 35 Antibacterial Drugs
|
|
|
|
|
|
|
Penicillin G and Penicillin V Pharmacology and Therapeutics
Therapeutic uses
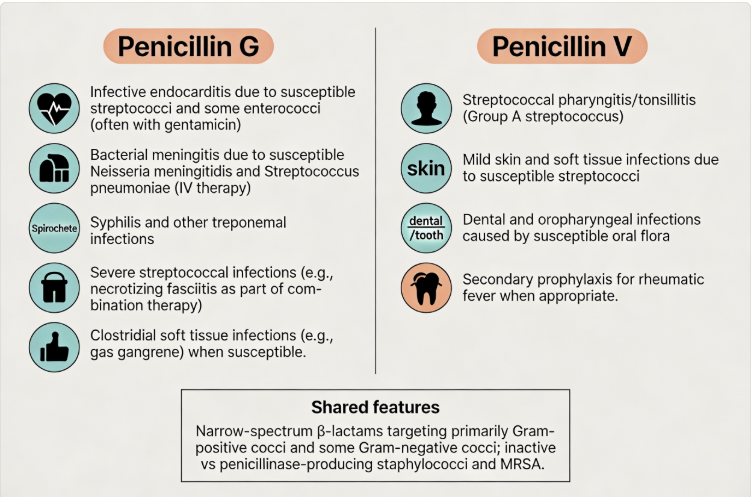 |
Serious Clostridial Infections
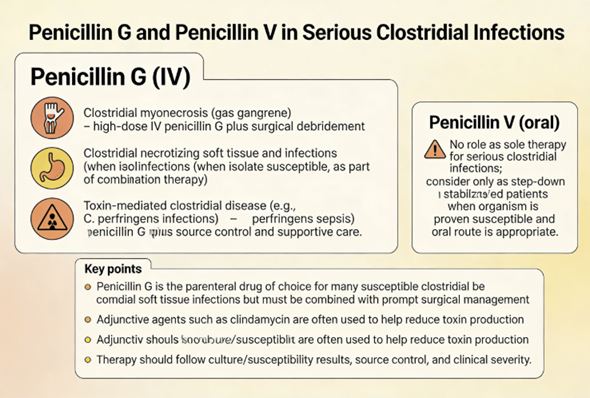 |
High-dose penicillin G along with surgical debridement is indicated for gas gangrene and Clostridium wound infections, as clostridial species (e.g. C. perfringens) are generally penicillin-susceptible.1
 |
|
For patients with suspected clostridial infection, empiric antibiotic treatment should not be delayed.
Some broad spectrum drugs used in this setting could include vancomycin, tazobactam, a carbapenem, or ceftriaxone with metronidazole.
However, if necrotizing soft tissue infection or gas gangrene is suspected, then penicillin in combination with clindamycin should be added, treating group A streptococcal necrotizing fasciitis.1
Penicillin G may be given IV in large doses for tetanus (caused by Clostridium tetani) as an adjunct to antitoxin, to eradicate the vegetative bacteria.
However, penicillin G which in the past was first-line treatment is now considered an acceptable alternative with metronidizole being the contemporary first-line treatment approach.
For patients with the history of serious allergic reactions to penicillin or metronidazole, desensitization of the patient to penicillin may be appropriate before trying alternatives.
Penicillin G is also used for botulism (wound botulism) as adjunct therapy after antitoxin, botulinum antitoxin, heptavalent (Rx).3
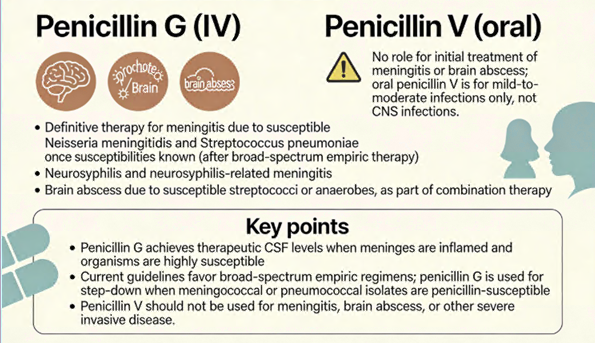 |
Penicillin G can treat meningococcal meningitis (caused by Neisseria meningitidis) if the strain is penicillin-susceptible.4
Initial empiric treatment (prior to susceptibility testing) would likely include an extended-spectrum cephalosporin, e.g. cefotaxime or ceftriaxone.
If the meningococcal isolate is susceptible to penicillin, treatment could be changed to penicillin G or ampicillin.
Alternatively, definitive treatment could also continue to utilize cefotaxime or ceftriaxone.4
At initial patient presentation meningitis due to Neisseria meningitidis may not be easily distinguished from other types of meningitis.5
![]() Therefore,
empirical treatment is important to initiate, given the
seriousness of the infection.
Therefore,
empirical treatment is important to initiate, given the
seriousness of the infection.
Another initial empirical therapeutic approach would include dexamethosone, ceftriaxone, cefotaxime (third-generation cephalosporins) and vancomycin.5
Acyclovir would be considered in accordance with the initial CSF evaluation.
Upon establishing at an accurate diagnosis of meningococcal meningitis, ceftriaxone or cefotaxime appears to be a drug of choice for treatment; moreover, penicillin G, ampicillin, chloramphenicol, fluoroquinolones, and aztreonam are described as alternative therapeutic approaches.5
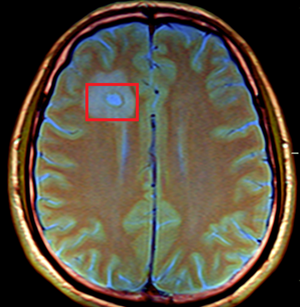
![]() Antibiotic
selection for treating brain abscess is challenging,
given the likelihood of polymicrobial presentations.6,7
Antibiotic
selection for treating brain abscess is challenging,
given the likelihood of polymicrobial presentations.6,7
 |
|
Therefore, empiric antibiotic therapy should cover oral streptococci, methicillin-susceptible staphylococci, anaerobes and Enterobacteriaceae.
Anaerobic coverage should also be considered.
Following culture, any initial empiric treatment protocol may be changed.
Streptococci coverage can be obtained with high-dose penicillin G or a third-generation cephalosporin (cefotaxime or ceftriaxone).
Metronidizole would be included to cover penicillin-resistant anaerobes.
If S. aureus is a concern, vancomycin may be utilized to address methicillin-resistant bacteria.6
August, 2025
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |